Heather Starmer Research Lab
Head & Neck Surgery

In addition to providing state of the art clinical care for communication and swallowing, our speech-language pathology team is engaged in clinical research to determine strategies to improve patient outcomes after a diagnosis of head and neck cancer. Our team recognizes the difficulties of going through cancer treatment and has particular interest in developing strategies to help patients make it through their treatment doing the therapies that will provide the best long-term outcomes. We collaborate closely with our surgeons, radiation oncologists, medical oncologists, and other team members to investigate how we can improve the patient experience of head and neck cancer care.
"Nothing would be more tiresome than eating and drinking if God had not made them a pleasure as well as a necessity.
— Voltaire
Our objective is to improve swallowing outcomes and patient satisfaction with swallowing after treatment for head and neck cancer.
Swallowing disorders are a common consequence of head and neck cancers and the treatments used to eradicate it. Swallowing issues may be related to the removal of structures in the mouth or throat, scarring or fibrosis of the mouth and throat, or swelling of the mouth, throat, or neck. Swallowing problems after head and neck cancer are cited as being the primary determinant of poor quality of life and may be associated with poor nutrition and development of aspiration pneumonia. Given this reality, our work seeks to identify practical strategies to minimize dysphagia and it’s complications.
Harnessing the Power of Technology
Technology has the potential to influence healthcare in many different ways. Approximately 10 years ago, Professor Starmer initiated work on a mobile application to support patients with head and neck cancer undergoing radiation therapy. This application, called The Head and Neck Cancer Virtual Coach™, provides patients with access to video workouts to perform to maintain the strength and mobility of their swallowing muscles, high-quality content about how to manage side effects during treatment, recipes and videos of foods that are well tolerated during treatment, and reminders to perform important therapy tasks. The impact of The Head and Neck Virtual Coach™ on patient outcomes and their experiences during treatment is currently under investigation at Stanford, Massachusetts Eye and Ear Infirmary, and the Fox Chase Cancer Center.
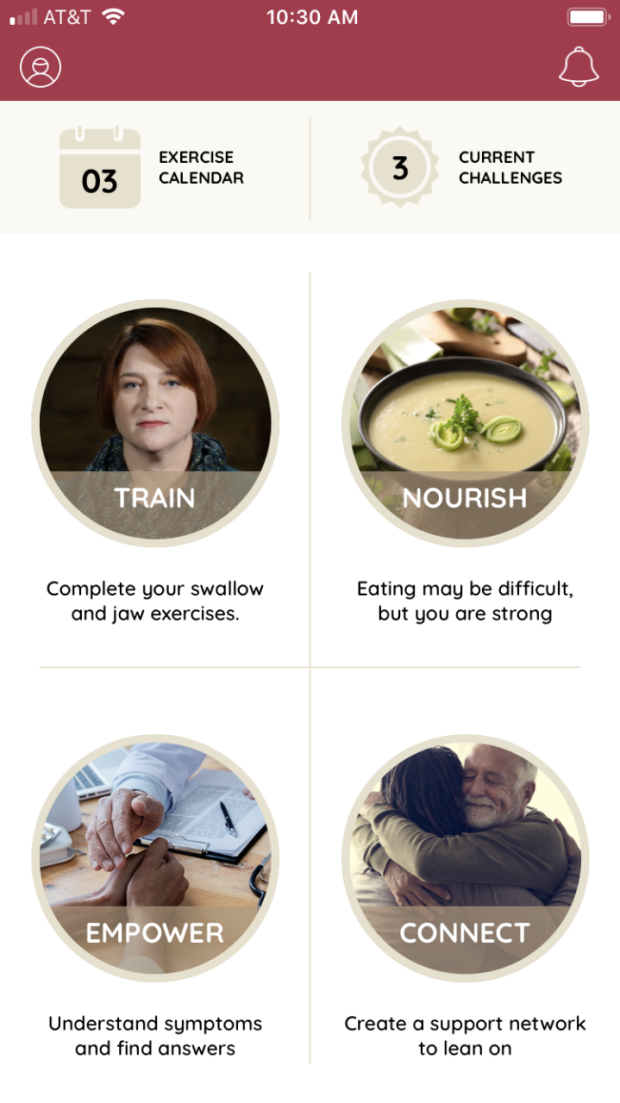
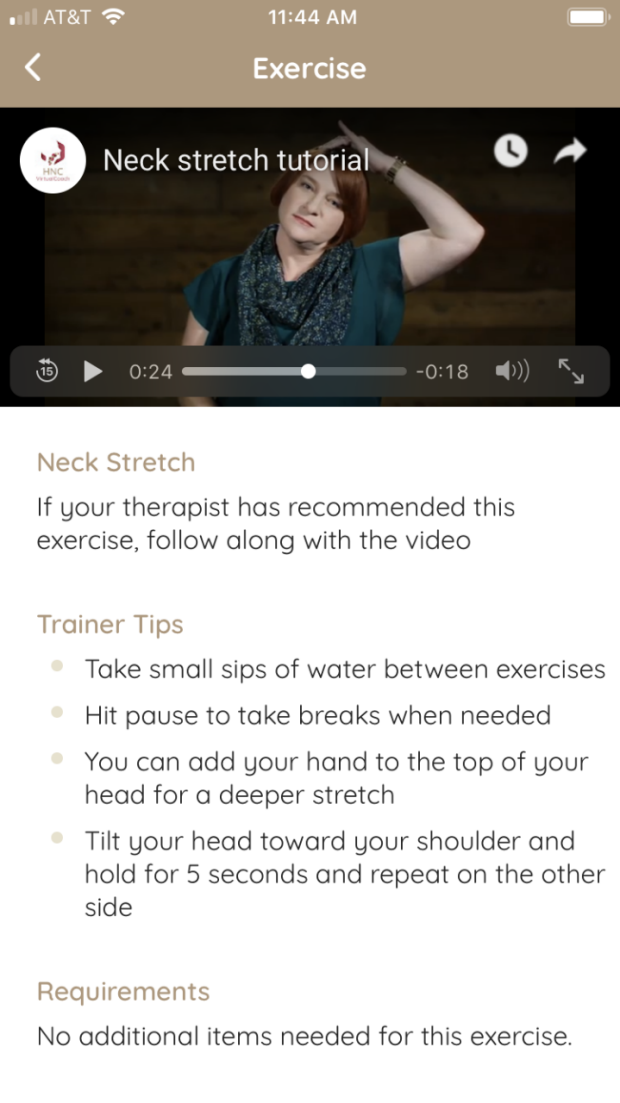
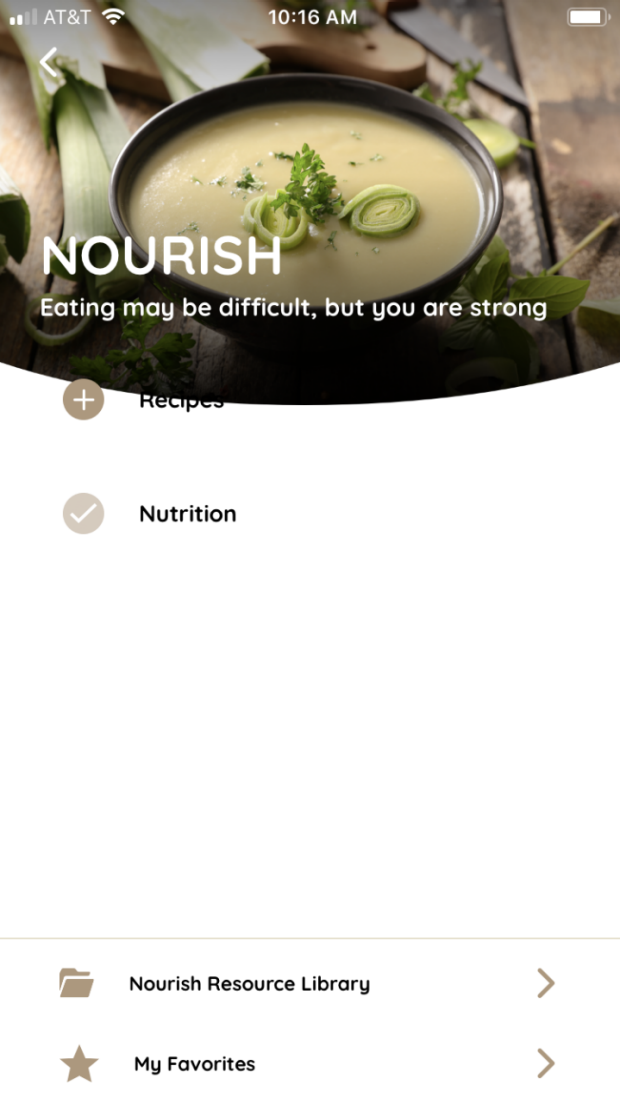
The Head and Neck Cancer Virtual Coach™ application screenshots.
Publication
Starmer HM, Klein D, Montgomery A, et al. Head and Neck Virtual Coach: A Randomized Control Trial of Mobile Health as an Adjunct to Swallowing Therapy During Head and Neck Radiation [published online ahead of print, 2022 Aug 12]. Dysphagia. 2022;10.1007/s00455-022-10506-5. doi:10.1007/s00455-022-10506-5.
Collaborators
- Jennifer Kizner (Stanford University)
- Jocelen Hamilton (Stanford University)
- Dr. Beth Beadle (Stanford University)
- Dr. F. Christopher Holsinger (Stanford University)
- Vibrent Health
- Dr. Jeremy Richmon (Massachusetts Eye and Ear Infirmary)
- Tessa Goldsmith (Massachusetts Eye and Ear Infirmary)
- Barbara Ebersole (Fox Chase Cancer Center)
Effective Treatment Requires Precision Diagnostics
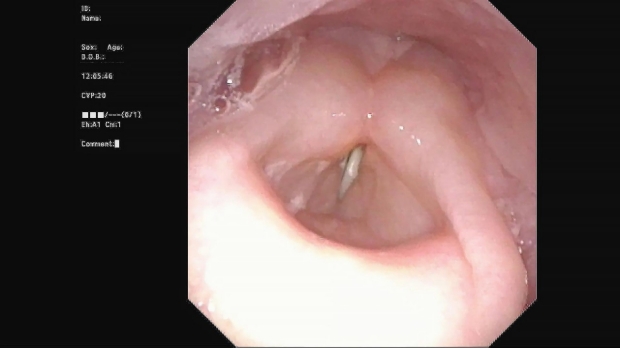
The ability to effectively manage swallowing disorders depends on diagnostic precision. Swallowing is typically evaluated using either fluoroscopy, an x-ray movie, or endoscopy. Both of these tools rely on an experienced clinician interpreting their images. Without use of reliable, standard rating systems, these interpretations can be subjective and lead to poorer patient outcomes and inadequate communication between clinicians. Further, research of advanced cancer treatments requires the ability to accurately assess the functional impact of the treatment. To address these challenges, our lab strives to establish and validate measurement tools to be used in patients with swallowing disorders. This work has resulted in the development of the DIGEST-FEES tool, which allows swallowing clinicians to reliably rate the safety and efficiency of an individual’s swallow using endoscopic assessment of swallowing.
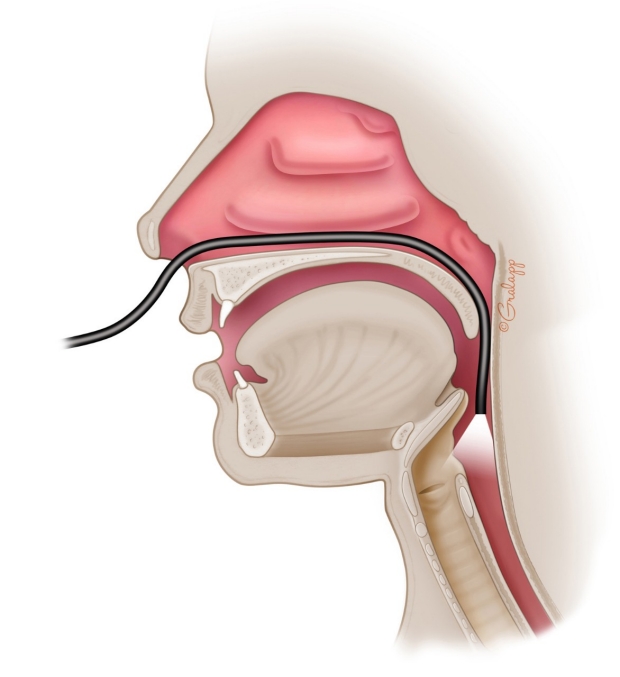
Endoscopic Evaluation.

Endoscopic Evaluation of Swallowing.
Collaborator
Dr. Katherine Hutcheson (MD Anderson Cancer Center)
Publications
ADAPTATION AND VALIDATION OF THE DYNAMIC IMAGING GRADE OF SWALLOWING TOXICITY FOR FLEXIBLE ENDOSCOPIC EVALUATION OF SWALLOWING: DIGEST-FEES. JOURNAL OF SPEECH, LANGUAGE, AND HEARING RESEARCH : JSLHR Starmer, H. M., Arrese, L., Langmore, S., Ma, Y., Murray, J., Patterson, J., Pisegna, J., Roe, J., Tabor-Gray, L., Hutcheson, K. 2021: 1-9
Abstract
Purpose While flexible endoscopic evaluation of swallowing (FEES) is a common clinical procedure used in the head and neck cancer (HNC) population, extant outcome measures for FEES such as bolus-level penetration-aspiration and residue scores are not well suited as global patient-level endpoint measures of dysphagia severity in cooperative group trials or clinical outcomes research. The Dynamic Imaging Grade of Swallowing Toxicity (DIGEST) was initially developed and validated for use during videofluoroscopic evaluations as a way to grade safety, efficiency, and overall pharyngeal swallowing impairment. The purpose of this study was to adapt and validate DIGEST for use with FEES. Method A modified Delphi exercise was conducted for content validation, expert consensus, adaptation, and operationalization of DIGEST-FEES. Three blinded, expert raters then evaluated 100 de-identified post-HNC treatment FEES examinations. Intra- and interrater reliability were tested with quadratic weighted kappa. Criterion validity against the MD Anderson Dysphagia Inventory, Functional Oral Intake Scale, Secretion Severity Scale, and Yale Residue Rating Scale was assessed with Spearman correlation coefficients. Results Interrater reliability was almost perfect for overall DIGEST-FEES grade (kappaw = 0.83) and safety grade (kappaw = 0.86) and substantial for efficiency grade (kappaw = 0.74). Intrarater reliability was excellent for all raters (0.9-0.91). Overall DIGEST-FEES grade correlated with MD Anderson Dysphagia Inventory (r = -.43, p < .0001), Functional Oral Intake Scale (r = -.43, p < .0001), Secretion Severity Scale (r = .47, p < .0001), Yale Vallecular Residue (r = .73, p < .0001), and Yale Pyriform Sinus Residue (r = .65, p < .0001). Conclusion DIGEST-FEES is a valid and reliable scale to describe the severity of pharyngeal dysphagia in patients with HNC. Supplemental Material https://doi.org/10.23641/asha.14642787.
View details for DOI 10.1044/2021_JSLHR-21-00014
View details for PubMedID 34033498
Lymphedema
Lymphedema can occur following surgery or radiotherapy for head and neck cancer. Internal lymphedema can contribute to swallowing, voice and breathing difficulties. Unlike external edema, there is no method currently available to measure internal edema. In conjunction with researchers in the United Kingdom, our lab is working to develop a scale that can be used to quantify the severity of internal edema impacting the throat and voice box.
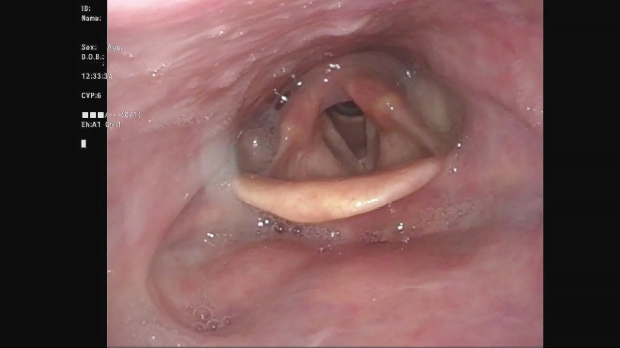
Normal Larynx
Laryngeal Edema
Collaborator
Dr Joanne Patterson (University of Liverpool)
Publications
Starmer, Heather, Mary Gemma Cherry, Joanne Patterson, Bridget Young, and Jason Fleming. “Assessment of Measures of Head and Neck Lymphedema Following Head and Neck Cancer Treatment: A Systematic Review.” Lymphatic Research and Biology, June 9, 2022, lrb.2021.0100. https://doi.org/10.1089/lrb.2021.0100.
DEVELOPMENT AND RELIABILITY OF THE REVISED PATTERSON EDEMA SCALE. CLINICAL OTOLARYNGOLOGY : OFFICIAL JOURNAL OF ENT-UK ; OFFICIAL JOURNAL OF NETHERLANDS SOCIETY FOR OTO-RHINO-LARYNGOLOGY & CERVICO-FACIAL SURGERY Starmer, H. M., Drinnan, M., Bhabra, M., Watson, L., Patterson, J. 2021
Abstract
OBJECTIVE: The Patterson Edema scale was developed in 2007 to address the lack of a reliable, sensitive scale to measure laryngeal and pharyngeal edema in patients with head and neck cancer. The objective of this study was to revise the existing Patterson scale to improve its reliability and utility.DESIGN: Prospective investigation SETTING: Academic medical center PARTICIPANTS: Speech-Language Pathologists, Otolaryngologists, and Radiation Oncologists MAIN OUTCOME MEASURES: Ratings using the Revised Patterson Edema Scale METHODS: A consensus group reviewed existing literature regarding the performance of the original Patterson scale and revised the existing scale in regard to items to be included and descriptors for each severity level. The scale was then utilized by 18 speech language pathologists from the US and UK with >2 years-experience working with dysphagia and dysphonia with endoscopy. Each SLP rated a total of eight parameters (epiglottis, vallecula, pharyngoepiglottic folds, aryepiglottic folds, arytenoids, false vocal folds, true vocal folds, and pyriform sinuses) using the Revised Patterson Edema Scale. Feedback was solicited from raters regarding areas where clarity was lacking for further scale revision. Scale revisions were completed and additional ratings were completed by otolaryngologists, radiation oncologists, and less experienced SLP providers to establish reliability across disciplines. Quadratic weighted Kappa values were obtained to establish interrater reliability.RESULTS: Feedback received from raters included suggestions for clarification of how to rate unilateral edema, use of a standard task battery to visualize and rate structures consistently, and clarification of true vocal fold edema rating parameters. Overall interrater reliability was established using quadratic weighted Kappa with good agreement noted for the epiglottis, vallecula, arytenoids, andfalse vocal folds; moderate agreement noted for aryepiglottic folds, pharyngoepiglottic folds and pyriform sinuses; and fair agreement noted for true vocal folds.CONCLUSIONS: The Revised Patterson Edema Scale demonstrates moderate-substantial interrater reliability for most parameters across multiple disciplines and experience levels, with the exception of the true vocal folds where agreement was fair. We believe the Revised Patterson Edema Scale provides a reliable tool for clinicians and researchers to rate edema in the supraglottic larynx and pharynx following treatment for head and neck cancer.
View details for DOI 10.1111/coa.13727
View details for PubMedID 33529494
Bio
Publications
-
Patient Experience of Head and Neck Surgery With Free Flap Reconstruction.
JAMA otolaryngology-- head & neck surgery
2024
More
Abstract
Importance: Major head and neck surgery with microvascular free tissue transfer reconstruction is complex, with considerable risk of morbidity. Little is known about patients' experiences, including decision-making prior to, and regret following, free flap surgery.Objective: To characterize patient experiences and decision regret of patients undergoing head and neck reconstructive free flap surgery.Design, Setting, and Participants: This mixed-methods cohort study comprising semistructured interviews was conducted June to August 2021 at a single tertiary academic cancer center. Participants underwent head and neck reconstructive surgery with microvascular free tissue transfer (flap) more than 3 months before recruitment (range, 3 months to 4 years). Interview transcripts were qualitatively analyzed for themes. Participants also completed a Decision Regret Scale questionnaire.Exposure: Microvascular free flap surgery for head and neck reconstruction.Main Outcomes and Measures: Thematic analysis of interviews, decision regret score.Results: Seventeen participants were interviewed. Median (IQR) age was 61 (52-70) years. Overall, 7 participants were women (49%), and 10 of 17 were men (59%). The most common free flap was fibula (8/17, 47%). Three major themes with 9 subthemes were identified: theme 1 was the tremendous effect of preoperative counseling on surgical decision-making and satisfaction, with subthemes including (1) importance of clinical care team counseling on decision to have surgery; (2) emotional context colors preoperative understanding and retention of information; (3) expectation-setting affects satisfaction with preoperative counseling; and (4) desire for diversified delivery of preoperative information. Theme 2 was coexisting and often conflicting priorities, including (1) desire to survive above all else, and (2) desire for quality of life. Theme 3 was perception of surgery as momentous and distressing, including (1) surgery as a traumatic event; (2) centrality of mental health, emotional resolve, and gratitude to enduring surgery and recovery; and (3) sense of accomplishment in recovery. On the Decision Regret Scale, most participants had no regret (n=8, 47%) or mild regret (n=5, 29%); 4 had moderate-to-severe regret (24%).Conclusions and Relevance: In this mixed-methods cohort study, patient experiences surrounding major head and neck reconstructive free flap surgery were described. Opportunities to improve support for this complex and vulnerable population, and to mitigate decision regret, were identified.
View details for DOI 10.1001/jamaoto.2023.4750
View details for PubMedID 38386356
-
Development of a head and neck lymphoedema specific quality of life tool: The Comprehensive Assessment of Lymphoedema Impact in the Head and Neck.
Head & neck
2024
More
Abstract
To develop a head and neck lymphoedema (HNL) specific quality of life (QoL) instrument to assess physical, functional, and social/emotional impacts of HNL.Instrument candidate items were reviewed by patients with HNL and clinicians and rated for importance, clarity, and invasiveness. The Content Validity Ratio was applied for item reduction. Three-step cognitive interviews were conducted with HNL patients to validate the items, survey format, and instructions.Initially, 130 candidate questions were developed. Following item reduction, 52 items progressed to three-step cognitive interviews. Following cognitive interviews, the Comprehensive Assessment of Lymphoedema Impact in Head and Neck (CALI-HaN) included 33 items; 1 global, 10 physical, 7 functional, and 15 emotional.Physical, functional, and socioemotional effects need to be considered when measuring QoL in patients with HNL. This study describes initial development of the CALI-HaN, an instrument that shows promise for clinical and research applications following future validation.
View details for DOI 10.1002/hed.27704
View details for PubMedID 38380786
-
Head and neck lymphedema and quality of life: the patient perspective.
Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer
2023; 31 (12): 696
More
Abstract
PURPOSE: Head and neck lymphedema (HNL) is common after head and neck cancer (HNC). This study aimed to explore quality of life (QoL) in patients with HNL to guide the development of a patient-reported QoL measure.METHODS: We conducted semi-structured interviews with 22 HNC survivors with HNL. Interviews explored participants' experiences of living with HNL. Analysis of interview transcripts drew on qualitative content analysis to ensure themes were grounded in patient experience.RESULTS: Two main themes were established: "I want to live my life" and "It was like things were short-circuited." These themes encompassed the substantial disruption patients attributed to the HNL and their desire to normalize life.CONCLUSIONS: Understanding the impact of HNL on individual patients may be critical to optimizing treatment strategies to improve the physical burden of HNL and QoL. This study provides the framework for developing a patient-reported HNL QoL measure.IMPLICATIONS FOR CANCER SURVIVORS: The development of an HNL-specific QoL measure, grounded in the patient perspective, may provide cancer care teams with a tool to better understand HNL's impact on each patient to tailor patient-centered care and optimize QoL outcomes.
View details for DOI 10.1007/s00520-023-08150-2
View details for PubMedID 37962667
-
Use of the G8 Geriatric Screening Tool in Surgical Head and Neck Cancer Patients Requiring Rehabilitation: A Multisite Investigation.
The Annals of otology, rhinology, and laryngology
2023: 34894231191869
More
Abstract
OBJECTIVES: The G8 is a well-validated screening test for older cancer patients. The current study was undertaken to determine whether the G8 is predictive of short-term post-operative outcomes after head and neck cancer (HNC) surgery.METHODS: Consecutive patients aged 65years or more and referred for a preoperative assessment by a speech-language pathologist were consecutively screened by clinicians at 2 academic medical centers using the G8. The G8 was used to screen for vulnerability prior to surgery. Patients were deemed vulnerable if they had a total G8 score ≤14 according to published guidelines. Data were also collected on demographic characteristics, tumor staging, post-operative course, and tracheostomy and feeding tube (FT) status.RESULTS: Ninety patients were consecutively screened during the study period. Using the G8, 64% of the patients were deemed vulnerable. Vulnerable patients differed significantly from non-vulnerable patients with regard to age, health, tumor stage, and baseline dysphagia, and underwent more extensive surgery. Postoperatively, vulnerable patients had a significantly longer hospital length of stay (LOS; 10.17 vs 5.50days, respectively, P<.001), were less likely to discharge home (76% vs 94%, P=.044), and were more likely to be FT dependent for over a month (54% vs 21%, P=.006) compared to non-vulnerable patients. In regression models, controlling for T-stage and surgical variables, the G8 independently predicted 2 post-operative outcomes of interest, namely LOS and FT dependency.CONCLUSIONS: The G8 may be a useful screening tool for identifying older adults at risk of a protracted postoperative medical course after HNC surgery. Future research should aim to identify the optimal screening protocol and how this information can be incorporated into clinical pathways to enhance the post-operative outcomes of older HNC patients.
View details for DOI 10.1177/00034894231191869
View details for PubMedID 37551009
-
Expert Consensus Statement: Management of Dysphagia in Head and Neck Cancer Patients.
Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery
2023; 168 (4): 571-592
More
Abstract
To develop an expert consensus statement (ECS) on the management of dysphagia in head and neck cancer (HNC) patients to address controversies and offer opportunities for quality improvement. Dysphagia in HNC was defined as swallowing impairment in patients with cancers of the nasal cavity, paranasal sinuses, nasopharynx, oral cavity, oropharynx, larynx, or hypopharynx.Development group members with expertise in dysphagia followed established guidelines for developing ECS. A professional search strategist systematically reviewed the literature, and the best available evidence was used to compose consensus statements targeted at providers managing dysphagia in adult HNC populations. The development group prioritized topics where there was significant practice variation and topics that would improve the quality of HNC patient care if consensus were possible.The development group identified 60 candidate consensus statements, based on 75 initial proposed topics and questions, that focused on addressing the following high yield topics: (1) risk factors, (2) screening, (3) evaluation, (4) prevention, (5) interventions, and (6) surveillance. After 2 iterations of the Delphi survey and the removal of duplicative statements, 48 statements met the standardized definition for consensus; 12 statements were designated as no consensus.Expert consensus was achieved for 48 statements pertaining to risk factors, screening, evaluation, prevention, intervention, and surveillance for dysphagia in HNC patients. Clinicians can use these statements to improve quality of care, inform policy and protocols, and appreciate areas where there is no consensus. Future research, ideally randomized controlled trials, is warranted to address additional controversies related to dysphagia in HNC patients.
View details for DOI 10.1002/ohn.302
View details for PubMedID 36965195
For Donors

Have a question?
Want to make a different type of gift or a larger contribution?
Please Contact
Cliff Harris
Director of Development
(650) 721-5659
ciharris@stanford.edu
Visit Stanford Medical Center Development to learn more about Endowments, Fellowships, and other giving opportunities.
Our Sponsors