Multidisciplinary Head & Neck Cancer Care
Head & Neck Surgery
We are the pioneers of major scientific breakthroughs
- Organ preservation approaches to head and neck cancer.
- New drugs for head and neck squamous cell carcinoma (HNSCC) and extending uses of existing drugs to HNSCC and nasopharyngeal carcinoma (NPC).
- Advanced radiation therapy techniques that limit toxicity and improve outcomes.
- Minimally Invasive and Robotic Surgery
- Stem cell work that extends the findings of the first paper, demonstrating the existence of “cancer stem cells” in HNSCC by researchers from Stanford and Michigan in 2007; and a 2009 Stanford study establishing that stem cell properties of patients’ malignancies correlate with prognosis. This work led to subsequent stem cell papers in 2011 and 2012.
- Normal tissue stem cell studies to identify salivary gland stem cells and to manipulate them for preservation and/or restoration of salivary gland function from radiation damage.
- HNOP’s breadth of research studies and protocols including treatment of intermediate and advanced disease as well as hypoxia imaging.
Our Innovations
- Creation of the first head and neck multidisciplinary tumor patient conference (tumor board; 1976) in the U.S.
- Introduction of the first use of chemotherapy with irradiation for head and neck squamous cell carcinoma (HNSCC), which is the basis of organ-preservation chemoradiation in the U.S.
- Close working relationships with:
- Neurosurgery, Interventional Radiology, and Neuroradiology,which are critical for complex open and endonasal endoscopic skull base surgery.
- Endocrinology in the treatment of thyroid cancer.
- Dermatology in the treatment of advanced skin cancers.
- Innovative research by physicians now at Stanford that demonstrates the utility of the FDA-approved Mobetron for intraoperative radiation therapy.
- Contributing research in a Phase II trial of immunotherapy in intermediate and advanced surgically-treated HNSCC. A Phase III trial is now planned.
- Leadership in the head and neck disease site committee of the Radiation Therapy Oncology Group to develop new nation-wide clinical trials in head and neck cancer.
- Biomarker studies to identify novel circulating biomarkers for prognostication and post-treatment surveillance in head and neck cancer.
- Strong links to developmental therapeutics such as the advancement of new drugs to treat cancer.
- Provision of a full range of treatment options that include minimally invasive surgery, robotic surgery, stereotactic radiosurgery such as CyberKnife, microvascular reconstruction, intraoperative radiation therapy (IORT), and new chemotherapy trials.
What is Head & Neck Cancer?
Head and neck cancer is a term that can include the broad array of tumors which may arise in this anatomically diverse region of the human body. Most often, the term head and neck cancer refers to tumors that arise from “squamous” cells that line the moist, mucosal surfaces of the mouth and throat. In fact, 95% of head and neck tumors are squamous cell carcinoma.
Tumors of the thyroid, salivary, and parathyroid glands, as well as cancers of the brain, nose and paranasal sinuses, esophagus, and eye, are not usually categorized as head and neck cancer. Furthermore, tumors of the skin, muscle and bone arising in the head and neck are also typically not included in this term.
Head and neck cancer is then further classified by its location within the mouth and throat:
Oral cavity
The lips, the oral tongue” (the forward two-thirds or front part of the tongue), the gums lining the upper and lower jaws, as well as the lining inside the cheek. The area known as the floor of the mouth is a mobile area between the lower jaw and gum and the oral tongue. The roof of the mouth or “hard palate” is also included as part of the oral cavity. Finally, a small triangulated area of mucosa or gum lining the area behind the last wisdom tooth is called the“retromolar trigone” and is also part of the oral cavity.
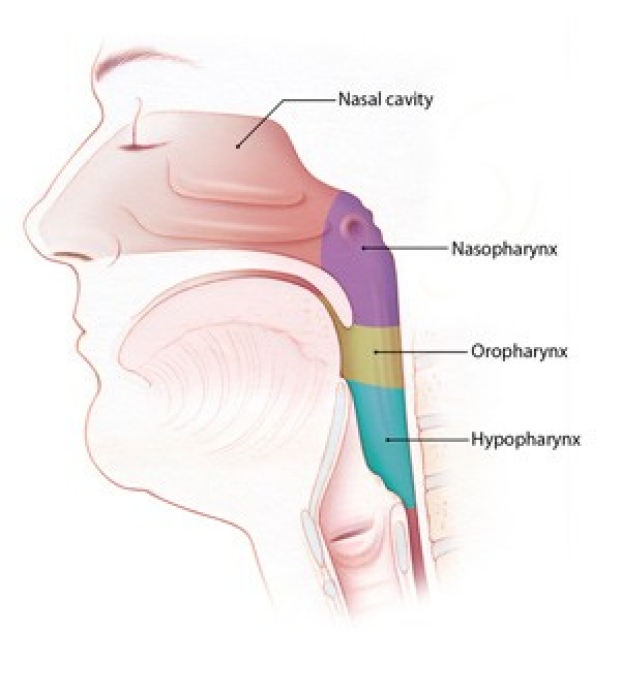
Pharynx
In medical terminology, the throat is known as the pharynx. In fact, the pharynx is supple tube or funnel that connects both the nose and mouth to the swallowing tube or esophagus. The pharynx is composed of three parts: the nasopharynx (the area just behind the nose); the oropharynx (behind the oral cavity and in the back of the mouth], and the hypopharynx, which surrounds the voice box and leads into the esophagus.
The larynx critical not only for the production of speech, but also breathing and swallowing. The “supraglottic” larynx has a valve called the epiglottis, which covers the larynx during swallowing to prevent “aspiration” of food into the lungs.

Treatments
HNOP offers multi-disciplinary, collaborative and integrated evaluation and care for patients with head and neck cancers.
Minimally invasive or endoscopic head and neck surgery (eHNS) is a dynamic new approach that allows surgeons to remove tumors with use of a specialized endocopes and cameras without external incisions and usually with little or no change in speech, appearance, and swallowing function.
An endoscope is a long, thin tube with special lighting and a narrow lens through which the surgeon can view organs and tissue inside of the body. For throat cancers, the surgeon inserts the endoscope through the patient’s mouth, and a microscope provides an excellent image of the tumor. Using very precise, state-of-the-art surgical instruments that are also inserted through the mouth, the surgeon can perform the operation without an external incision.
eHNS has several advantages in many cases. Some of these advantages are:
- Reduced risk of blood loss
- Lower pain levels
- Fewer days spent in the hospital
- Quicker return to a normal diet and faster recovery time
- Less scarring, with improved cosmetic appearance
In some cases of throat cancer, eHNS may reduce or even eliminate the need for chemotherapy and radiation therapy.
At Stanford, your team of surgeons, oncologists, and radiologists will work together to determine the best course of action for you. The goal with eHNS is always the same: to eliminate the cancer while minimizing the risks and recovery time associated with traditional cancer care.
Chemotherapy or radiation therapy may still be necessary after eHNS. When chemotherapy and radiation therapy cannot be avoided through surgery, eHNS may still hold advantages for patients. Faster recovery after eHNS means patients can usually begin chemotherapy and radiation therapy earlier. And the smaller incisions with eHNS heal more quickly than larger incisions and are less likely to become infected.
Two types of eHNS, transoral robotic surgery (TORS) and transoral laser CO2microsurgery (TLM), have revolutionized the treatment for throat cancer.
Robotic surgery uses state-of-the-art technology that allows surgeons to safely remove certain thyroid tumors through discrete incisions several inches from the neck. Because no incision is made in the neck, the patient avoids a neck scar.
The da Vinci ® surgical system is a highly sophisticated computerized system that is used for robotic thyroid surgery. The surgeon cuts a 1-inch to 2-inch incision in the folds of skin under the patient’s arm and inserts the da Vinci ® system’s robotic arms, which have been customized to resemble standard surgical instruments. The surgeon guides the robotic arms underneath the skin toward the thyroid gland.
The surgeon views the surgical field on a 3-D high-definition screen, magnified up to 10 times. The skilled surgeons at Stanford Medicine control the da Vinci ® system’s robotic arms as one might control conventional surgery. The instruments on the robotic arms can move with seven degrees of movement and rotate 540 degrees, giving the surgeon the ability to manipulate delicate tissues with precision.
Robotic thyroidectomy is not available for all thyroid tumors. If your thyroid tumor is less than 3 cm in size and is likely to be benign (non-cancerous), then robotic surgery may be an option. Your surgeons will help you decide the best approach for you.
Neoadjuvant Atezolizumab in Surgically Resectable Advanced Cutaneous Squamous Cell Carcinoma
The purpose of this research is to evaluate whether the administration of atezolizumab before surgical resection of your tumor is feasible and to evaluate the treatment response, safety, and tolerability of atezolizumab.
Stanford is currently not accepting patients for this trial.
Stanford Investigator(s):
Intervention(s):
- drug: Atezolizumab
Eligibility
Inclusion Criteria:
1. Signed Informed Consent Form
2. Age ³ 18 years at time of signing Informed Consent Form
3. Histologically or cytologically confirmed squamous cell carcinoma
4. Measurable disease per RECIST v1.1
- Note that protocol specified imaging is not necessary to fulfill this criterion.
For example, a patient presenting with a visible 4cm primary lesion who has
obviously RECIST evaluable disease may be considered eligible prior to baseline
imaging stipulated in the protocol.
5. Availability of a representative tumor specimen that is suitable for determination of
PD-L1 immunohistochemical stain evaluation.
6. Eastern Cooperative Oncology Group (ECOG) Performance Status of 0 or 1
7. Adequate hematologic and end-organ function appropriate for surgery as determined by
routine preoperative evaluation. If liver function, renal function and hematologic
laboratory test results are within limits acceptable for elective surgery. Laboratory
results that will need to be obtained within 28 days prior to initiation of study
treatment:
- aspartate aminotransferase (AST), alanine aminotransferas (ALT), total bilirubin,
and alkaline phosphatase (ALP) £ 2.5 x upper limit of normal (ULN.).
- Thyroid-stimulating hormone (TSH) < 13, Patients with a history of a high TSH who
are receiving levothyroxine replacement at the time of eligibility evaluation and
have no clinical evidence of hypothyroidism are eligible.
8. For patients receiving therapeutic anticoagulation: stable anticoagulant regimen
9. Negative hepatitis B surface antigen (HBsAg) test at screening
10. For women of childbearing potential: agreement to remain abstinent (refrain from
heterosexual intercourse) or use contraceptive methods, as defined below: Women must
remain abstinent or use contraceptive methods with a failure rate of < 1% per year
during the treatment period and for 5 months after the final dose of atezolizumab.
A woman is considered to be of childbearing potential if she is postmenarchal, has not
reached a postmenopausal state (³ 12 continuous months of amenorrhea with no
identified cause other than menopause), and has not undergone surgical sterilization
(removal of ovaries and/or uterus). The definition of childbearing potential may be
adapted for alignment with local guidelines or requirements.
Examples of contraceptive methods with a failure rate of < 1% per year include
bilateral tubal ligation, male sterilization, hormonal contraceptives that inhibit
ovulation, hormone-releasing intrauterine devices, and copper intrauterine devices.
The reliability of sexual abstinence should be evaluated in relation to the duration
of the clinical trial and the preferred and usual lifestyle of the patient. Periodic
abstinence (e.g., calendar, ovulation, symptothermal, or postovulation
11. For men: Agreement to remain abstinent (refrain from heterosexual intercourse) or use
a condom, and agreement to refrain from donating sperm, as defined below:
With a female partner of childbearing potential or pregnant female partner, men must agree
to remain abstinent or use a condom during the treatment period and for 5 months after the
final dose of atezolizumab to avoid exposing the embryo. Men must agree to refrain from
donating sperm during this same period
Exclusion Criteria:
1. Patients not eligible for standard of care surgical resection
2. Distant metastatic disease
3. Uncontrolled pleural effusion, pericardial effusion, or ascites requiring recurrent
drainage procedures (once monthly or more frequently)
- Patients with indwelling catheters (e.g., PleurX are allowed.
4. Uncontrolled or symptomatic hypercalcemia (ionized calcium > 1.5 mmol/L, calcium > 12
mg/dL or corrected serum calcium > ULN)
5. Active or history of autoimmune disease or immune deficiency, including, but not
limited to, myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus
erythematosus, rheumatoid arthritis, inflammatory bowel disease, antiphospholipid
antibody syndrome, Wegener granulomatosis, Sjögren syndrome, Guillain-Barré syndrome,
or multiple sclerosis (see Appendix G for a more comprehensive list of autoimmune
diseases and immune deficiencies), with the following exceptions: ·Patients with a
history of autoimmune-related hypothyroidism who are on thyroid-replacement hormone
are eligible for the study.
·Patients with controlled Type 1 diabetes mellitus who are on an insulin regimen are
eligible for the study.
·Patients with eczema, psoriasis, lichen simplex chronicus, or vitiligo with
dermatologic manifestations only (e.g., patients with psoriatic arthritis are
excluded) are eligible for the study provided all of following conditions are met:
- Rash must cover < 10% of body surface area
- Disease is well controlled at baseline and requires only low-potency topical
corticosteroids
- No occurrence of acute exacerbations of the underlying condition requiring
psoralen plus ultraviolet A radiation, methotrexate, retinoids, biologic agents,
oral calcineurin inhibitors, or high-potency or oral corticosteroids within the
previous 12 months
6. History of idiopathic pulmonary fibrosis, organizing pneumonia (e.g., bronchiolitis
obliterans), drug-induced pneumonitis, or idiopathic pneumonitis, or evidence of
active pneumonitis on screening chest computed tomography (CT) scan ·History of
radiation pneumonitis in the radiation field (fibrosis) is permitted.
7 .Active tuberculosis. Patents do NOT have to be screened for tuberculosis for this trial.
8. Significant cardiovascular disease (such as New York Heart Association Class II or
greater cardiac disease, myocardial infarction, or cerebrovascular accident) within 3
months prior to initiation of study treatment, unstable arrhythmia, or unstable angina 9.
Severe infection within 4 weeks prior to initiation of study treatment, including, but not
limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia
10. Treatment with therapeutic oral or IV antibiotics within 2 weeks prior to initiation of
study treatment
- Patients receiving prophylactic antibiotics (e.g., to prevent a urinary tract
infection or chronic obstructive pulmonary disease exacerbation) are eligible for the
study. 11. Prior allogeneic stem cell or solid organ transplantation 12. Any other
disease, metabolic dysfunction, physical examination finding, or clinical laboratory
finding that contraindicates the use of an investigational drug, may affect the
interpretation of the results, or may render the patient at high risk from treatment
complications 13. Treatment with a live, attenuated vaccine within 4 weeks prior to
initiation of study treatment, or anticipation of need for such a vaccine during
atezolizumab treatment or within 5 months after the final dose of atezolizumab 14.
Current treatment with anti-viral therapy for hepatitis B virus (HBV) 15. Treatment
with investigational therapy within 28 days prior to initiation of study treatment 16.
Prior treatment with CD137 agonists or immune checkpoint blockade therapies, including
anti- cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), anti-PD-1, and anti-PD-L1
therapeutic antibodies 17. Treatment with systemic immunostimulatory agents
(including, but not limited to, interferon and interleukin 2 [IL-2]) within 4 weeks or
5 half-lives of the drug (whichever is longer) prior to initiation of study treatment
18. Treatment with systemic immunosuppressive medication (including, but not limited
to, corticosteroids, cyclophosphamide, azathioprine, methotrexate, thalidomide, and
anti-tumor necrosis factor (TNF)-a agents) within 2 weeks prior to initiation of study
treatment, or anticipation of need for systemic immunosuppressive medication during
study treatment, with the following exceptions:
- Patients who received acute, low-dose systemic immunosuppressant medication or a
one-time pulse dose of systemic immunosuppressant medication (e.g., 48 hours of
corticosteroids for a contrast allergy) are eligible for the study has been obtained.
- Patients who received mineralocorticoids (e.g., fludrocortisone), corticosteroids for
chronic obstructive pulmonary disease (COPD) or asthma, or low-dose corticosteroids
for orthostatic hypotension or adrenal insufficiency are eligible for the study. 19.
History of severe allergic anaphylactic reactions to chimeric or humanized antibodies
or fusion proteins 20. Known hypersensitivity to Chinese hamster ovary cell products
or to any component of the atezolizumab formulation 21. Pregnancy or breastfeeding, or
intention of becoming pregnant during study treatment or within 5 months after the
final dose of study treatment
- Women of childbearing potential must have a negative serum pregnancy test result
within 14 days prior to initiation of study treatment.
Ages Eligible for Study
18 Years - N/A
Genders Eligible for Study
All
Not currently accepting new patients for this trial
Contact Information
Stanford University
School of Medicine
300 Pasteur Drive
Stanford,
CA
94305
Team Head and Neck
secure-headandneckresearch@lists.stanford.edu
Not Recruiting