Annual Report 2019
• Stopping cancer in its tracks
• SOAR Residency Program lays foundation for independent research careers
• Creating a field of molecular surgery to guide new therapies
> Developing cures with stem cells and regenerative medicine
Developing cures with stem cells and regenerative medicine

Albert Wu, MD, PhD, FACS, uses patients’ own cells in an effort to create personalized treatment options.
Too many major eye diseases lead to loss of vision that, even with current medicine or surgery, is irreversible. In macular degeneration, glaucoma, and the major corneal diseases, the cells responsible for normal visual function die and are not replaced through natural healing mechanisms. Researchers in the Department of Ophthalmology at Stanford are seeking to reverse this limitation through development and testing of groundbreaking stem cell and regenerative medicine therapies.
“Our goal is to stabilize, better diagnose, and find cures for common eye diseases, so that we can help not just our patients, but patients globally as well,” said Jeffrey Goldberg, MD, PhD, professor and chair of ophthalmology at Stanford, noting that some 1.3 billion people worldwide suffer from vision impairment. “Restoring vision in these diseases has become a major focus for our research at Stanford.”
Department faculty are now paving the way in battling vision loss through stem cell research focused on diseases that range from the cornea on the front of the eye to the retina and optic nerve in the back.
.jpeg)
Wu’s research aimed at recreating ocular stem cells shows a paraffin-embedded section of developing human eyelid tissue stained with cytokeratin-14 immunofluorescence.
Repairing the cornea
The cornea’s outer surface is covered with a layer of epithelial cells that are constantly sustained and replenished by stem cells that normally live in a specialized niche at the edge of the cornea called the limbus. However, in chemical burns, severe infections, and certain immune system diseases such as Stevens-Johnson Syndrome, these limbal stem cells are depleted and the corneal epithelium degenerates, leading to significant visual impairment. Replacing limbal stem cells with advanced tissue transplant surgery has long been a strength at the Byers Eye Institute, critical to patient care in these devastating diseases, but simplifying such tissue transplants with a limbal stem cell replacement therapy could provide a safer, more durable approach while broadening patient access.
Albert Wu, MD, PhD, FACS, assistant professor of ophthalmology, is pushing this approach further by developing ways to regenerate a patient’s damaged corneal tissue with stem cells created directly from that patient’s blood or skin. Using the patient’s own cells, rather than donor cells, vastly decreases the chance of immune rejection. Wu, who joined the department at the end of 2017, now serves as the director of oculoplastics research at Stanford, where he heads the Ophthalmic Stem Cell and Regenerative Medicine Laboratory.
Wu’s research on recreating ocular stem cells from a patient’s cells began with a five-year National Eye Institute grant, and at Stanford he has received philanthropic support to accelerate this research. He is also advancing Stanford’s deep strengths in stem cell biology by collaborating with Irving Weissman, MD, director of the Stanford Institute for Stem Cell Biology and Regenerative Medicine, and Marius Wernig, MD, associate professor of pathology and a member of this institute. They are currently studying how stem cells are converted into ocular tissue and how they interact with their local environment, and moving this research into models for preclinical testing.
“My goal is to perform translational research, bringing breakthroughs in stem cell biology and tissue engineering to clinical ophthalmology and reconstructive surgery,” Wu said.
The innermost layer of the cornea presents a similar challenge. There, a fragile layer of corneal endothelial cells can degenerate with age, after cataract or other eye surgery, or in genetic diseases such as Fuch’s dystrophy, and in humans they are not repaired or replaced endogenously. These cells are responsible for pumping fluid out of the cornea and, in so doing, keep the cornea clear. Their loss leads to visual decline and, in some cases, severe pain that can only be treated with surgery.
“Partial thickness corneal transplants such as Descemet stripping automated endothelial keratoplasty (DSAEK) and Descemet membrane endothelial keratoplasty (DMEK) can fix the problem, but it would be even better to have cell-based therapies that could help more patients,” said Charles Lin, MD, clinical assistant professor of ophthalmology and a leader in complex cornea transplant surgery.
Delivering corneal endothelial cell therapies could help avoid surgery altogether. With a grant from the California Institute for Regenerative Medicine, Goldberg worked on converting human stem cells derived from adult patients into corneal endothelial cells. He previously showed that using magnetic nanoparticles and external magnets could help deliver corneal endothelial cells to the right spot inside the eye. After growing new corneal cells, the cells are then placed toward the inside of the cornea and held in place by the magnet.
Lin is excited to move this type of research into clinical trials.
“Generating cells for thousands of patients is particularly important when considering the worldwide shortage of access to corneal transplant surgery,” Lin said.
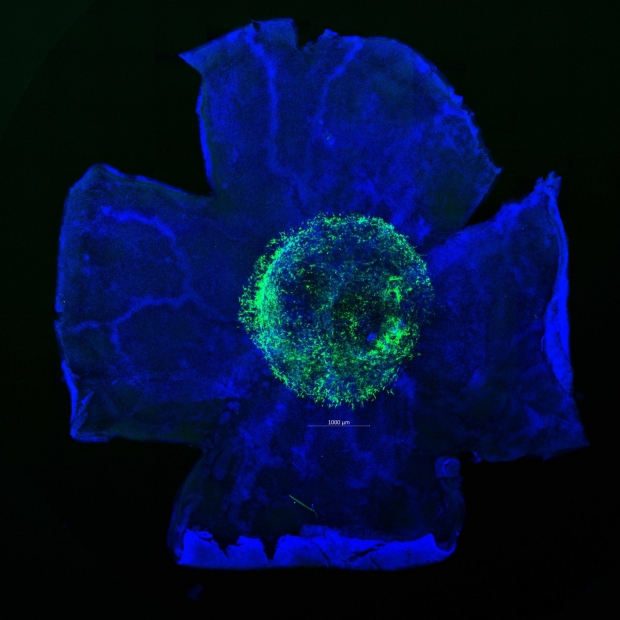
Green fluorescent protein-expressing retinal ganglion-like cells integrate after transplantation into a rodent eye.
Developing therapies for age-related macular degeneration
Within the department, there is also ongoing research aimed at treating age-related macular degeneration (AMD), a leading cause of vision loss for Americans 50 years and older, according to the National Eye Institute. AMD causes damage to the retina in two ways. In dry AMD, the more common form, the retinal pigment epithelial cells and the photoreceptors in the center of the retina atrophy and die. Wet AMD is less common, but more acutely vision threatening, and is associated with blood vessels that grow under the retina and leak or bleed. While there are successful treatment options for wet macular degeneration, an effective treatment for the cellular loss in dry macular degeneration has not been found, and both of these forms dramatically disrupt patients’ central vision. Theodore Leng, MD, assistant professor of ophthalmology, has focused his research on developing treatments for those with dry AMD.
“While this disease is a slow, progressive form of vision loss, patients can still eventually become blind from it,” Leng said.
Leng notes that a number of other retinal degenerative diseases, such as those associated with high levels of myopia, or nearsightedness, and other less common genetic diseases, are closely related and likely stand to benefit from cell therapies.
Leng has been the principal investigator in a number of clinical trials for dry AMD using cell therapies and other therapeutic candidates, and he remains optimistic in pursuing a cure. Recently, he was awarded a $4.2 million grant from the California Institute for Regenerative Medicine to develop a stem cell therapy for dry AMD. Leng and his collaborators are studying adult neural stem cells derived from brain tissue that can only become other cells within the central nervous system, and optimizing them for human clinical trials.
“These cells secrete growth factors and other supportive nutrients for the remaining nerve cells of the eye, so when we surgically implant them under the retina, they will live there and create a favorable environment for the other cells in the retina,” Leng said.
Other cell replacement programs Leng is collaborating on are specifically designed to replace the retinal pigment epithelial cells, and the rod and cone photoreceptors.
“The hope is that we will move into human clinical trials in the next two to three years,” Leng said.
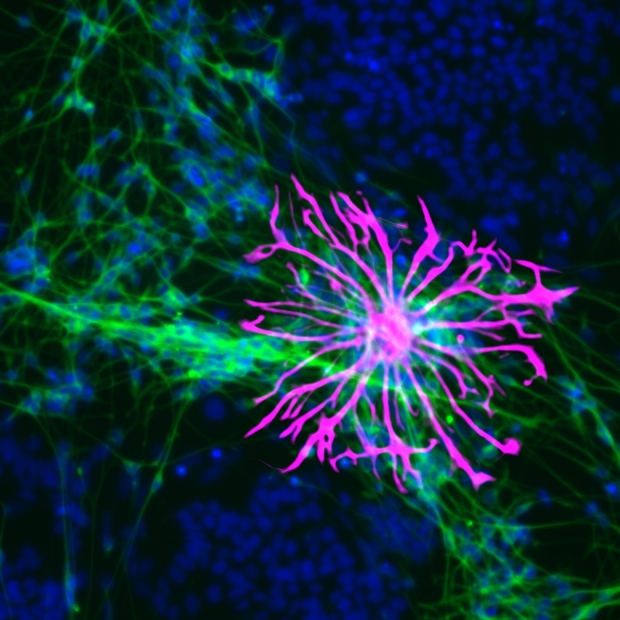
Retinal ganglion cells can be derived from human adult stem cells (green indicates neuronal cells, magenta indicates glial cells, and blue indicates nuclei).
Stem cells for glaucoma and optic nerve disease
In the retina, just a millimeter away from the retinal photoreceptors that degenerate in AMD, are the retinal ganglion cells, whose axon fibers carry visual information from the eye down the optic nerve to the brain. These neurons degenerate in glaucoma, as well as in other optic nerve degenerations such as with ischemia, or compression from tumors. Like other neurons in the retina and the brain, once they degenerate, there is no natural replacement, making retinal ganglion cells a strong candidate for cell replacement therapy. Great progress has been made in recent years in understanding how to differentiate stem cells into retinal ganglion cells in the laboratory, and in transplanting retinal ganglion cells into the retina.
“The challenge for cell therapy for glaucoma is even greater, because not only do the donor cells have to integrate into the retina, they have to regrow their axons to the brain,” Goldberg said.
A team of faculty at Stanford faculty is focused on exactly this challenge of optic nerve regeneration, including Yang Hu, MD, PhD, assistant professor of ophthalmology; Y. Joyce Liao, MD, PhD, associate professor of ophthalmology and neurology; Michael Kapiloff, MD, PhD, associate professor of ophthalmology and of medicine; Andrew Huberman, PhD, associate professor of ophthalmology and neurobiology; and Goldberg, who anticipates the application of approaches to promote optic nerve regeneration to his stem cell research for retinal ganglion cell replacement.
Looking to the future
Together, these programs have used the research and clinical environment at Stanford to accelerate progress toward cell therapies for otherwise untreatable conditions.
“Stanford has been great for facilitating the movement of science between the lab and clinic,” Wu said, noting the increase in clinical trials for regenerative therapies in the last few years.
“This stem cell research coming from the Wu, Leng, and Goldberg laboratories really showcases the deep commitment of this ophthalmology department to include stem cell biology approaches to find cures for currently incurable diseases of the eye,” Weissman said. “I am excited to see how these continued studies and advanced clinical trials can help return vision to patients.”
By KATHRYN SILL
Kathryn Sill is a web and communications specialist for the Byers Eye Institute in the Department of Ophthalmology, at Stanford University School of Medicine. Email her at ksill@stanford.edu.