Stanford Medicine researchers develop a new imaging method to create a cell-by-cell reconstruction of skin or other tissue without taking a biopsy.
April 10, 2024 - By Sarah C.P. Williams
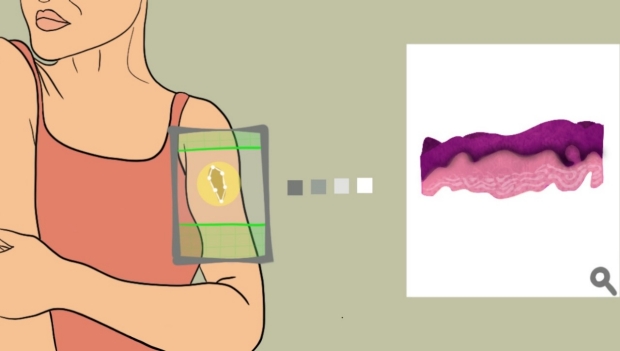
Stanford Medicine researchers have developed a method to penetrate tissue with lasers, creating a high-resolution, three-dimensional image of its cells.
Emily Moskal
The next time you have a suspicious-looking mole on your back, your dermatologist may be able to skip the scalpel and instead scan the spot with a noninvasive “virtual biopsy” to determine whether it contains any cancerous cells. Similarly, surgeons trying to determine whether they have removed all of a breast tumor may eventually rely on an image captured during surgery rather than wait for a pathologist to process the excised tissue.
Stanford Medicine researchers have developed a method that uses lasers to penetrate tissue and create a high-resolution, three-dimensional reconstruction of the cells it contains. From this virtual reconstruction, they can make cross-sectional images that mimic those generated by a standard biopsy, in which a sample of tissue is sliced into thin layers and placed on a slide to be examined under a microscope.
The new method, published April 10 in Science Advances, could be used to noninvasively scan the skin for unhealthy cells as well as provide rapid results on biopsies taken elsewhere in the body. It could also provide more information than current diagnostic approaches.
“We’ve not only created something that can replace the current gold-standard pathology slides for diagnosing many conditions, but we actually improved the resolution of these scans so much that we start to pick up information that would be extremely hard to see otherwise,” said Adam de la Zerda, PhD, an associate professor of structural biology and the senior author of the article describing the method.

Adam de la Zerda
The method was developed by Yonatan Winetraub, PhD, a former graduate student in the de la Zerda lab who now leads his own research lab at Stanford focusing in part on virtual biopsies.
“This has the potential to transform how we diagnose and monitor concerning skin lesions and diseases in the clinic,” added co-author Kavita Sarin, MD, PhD, an associate professor of dermatology.
Laser vision
When a dermatologist or surgeon takes a biopsy from someone’s body — whether from the skin, liver, breast or elsewhere — the tissue is usually sent to a pathologist, who slices the biopsied tissue into thin layers. The pathologist then stains each layer with chemicals called hematoxylin and eosin (H&E), which lets them more easily see the patterns, shapes and structures of cells. These H&E slides are routinely used for diagnosing cancers and other diseases. But the slides are labor intensive and are irreversible; once a biopsy is sliced in one direction, for instance, it cannot be sliced another way to provide a different view.
For nearly a decade, de la Zerda and his colleagues have been studying a different way of seeing inside the body, called optical coherence tomography. Typically used by ophthalmologists to image the back of the eye, OCT scans measure how light waves from a laser bounce off a tissue to create a rendering of its insides (similar to the way ultrasound uses sound waves to visualize organs).
As de la Zerda and Winetraub enhanced the OCT scans so they would work in organs other than the eye — developing both new hardware to collect data and new processing methods — they needed a way to verify the accuracy of their scans, so they sent the tissues they were scanning with OCT to pathologists to create H&E images.

Kavita Sarin
“We kept improving and improving the quality of the image, letting us see smaller and smaller details of a tissue,” de la Zerda explained. “And we realized the OCT images we were creating were really getting very similar to the H&Es in terms of what they could show.”
Help from artificial intelligence
The higher resolution of the OCT images opened the door to using the method to diagnose disease without producing H&Es. But de la Zerda and his colleagues thought clinicians would be more apt to use OCT if the images looked familiar.
“Every physician in a hospital is very much used to reading H&Es, and it was important to us that we translate OCT images into something that physicians were already comfortable with —rather than an entirely new type of image,” de la Zerda said.
Winetraub turned to artificial intelligence to help convert OCT scans into flat images resembling H&E slides.
For 199 skin biopsies collected at Stanford Hospital, Winetraub carried out an OCT scan before pathologists created H&E slices. He and his colleagues developed a way of putting molecular tags on the surface of the biopsies so they could be sure exactly where in the OCT scan each H&E slice came from. Then, Winetraub paired up 1,005 of these H&E images with the corresponding OCT images and entered them into an artificial intelligence algorithm which could learn how to create accurate H&Es from the raw OCT data.
“The uniqueness of this work lies in the method we developed to align OCT and H&E image pairs, letting machine-learning algorithms train on real tissue sections and providing clinicians with more accurate virtual biopsies,” Winetraub said.

Yonatan Winetraub
The researchers fine-tuned the AI program by showing it an additional 553 pairs of H&E and OCT images before testing it out on new OCT images. When three Stanford dermatologists analyzed random assortments of true H&E images and those created from the OCT scans, they could detect cellular structures at a similar rate. Any number of H&E images can be created from a single OCT image, virtually slicing the three-dimensional reconstruction in any direction.
Toward non-invasive biopsies
When a dermatologist notices an unusual looking spot on a person’s skin, they currently have two options to determine if it poses a risk: wait and see whether it grows bigger, or cut it off and send it to a pathologist for testing.
De la Zerda and Winetraub now see a third path — scanning a potentially cancerous mole with OCT and analyzing the virtual H&E images.
“Imagine if we could give physicians the ability, right there in the room with the patient, to take out an OCT camera and — rather than slice the patient up in dozens of places — image the cells inside each mole,” de la Zerda said.
Similarly, surgeons removing breast tumors currently send removed tissue to pathologists to process over several days and determine whether any cancerous cells were missed. Around 20% of breast cancer patients require a second surgery to remove more cells. If H&E images could be produced from an OCT camera in the operating room to instantaneously detect whether cancer cells remained, subsequent surgeries could be avoided.
More work is needed to move the approach toward these applications, but the researchers are confident that their approach will give clinicians a new way to carry out biopsies.
Funding for this research was provided by the United States Air Force, the National Institutes of Health (grants DP50D012179 and K23CA211793), the National Science Foundation, the Damon Runyon Cancer Research Foundation, the Claire Giannini Fund, the Susan G. Komen Breast Cancer Foundation, the Mary Kay Foundation, the Skippy Frank Foundation, the Donald E. and Delia B. Baxter Foundation, the Center for Cancer Nanotechnology Excellence and Translation, the Chan Zuckerberg Biohub, the Pew Charitable Trusts, the Alexander and Margaret Stewart Trust, the Damon Runyon Cancer Research Foundation, and Stanford Bio-X.
About Stanford Medicine
Stanford Medicine is an integrated academic health system comprising the Stanford School of Medicine and adult and pediatric health care delivery systems. Together, they harness the full potential of biomedicine through collaborative research, education and clinical care for patients. For more information, please visit med.stanford.edu.

