A search for medical needs in eye clinics led Stanford Biodesign fellows to develop an implantable neurostimulator that painlessly increases natural tear production.
January 23, 2015 - By Kris Newby
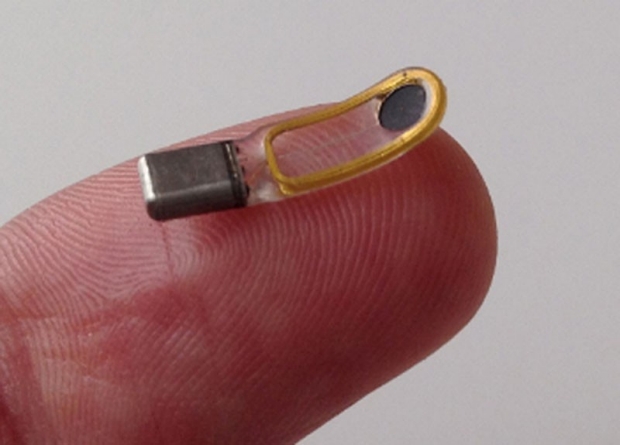
This wireless device is designed to stimulate natural tear production in patients with dry eye.
Michael Ackermann
Michael Ackermann, PhD, knows how to make you cry.
But this is a good thing for the more than 20 million Americans who suffer from a painful condition in which the lacrimal glands don’t create enough tears to lubricate the surface of the eye.
To help these patients, Ackermann, PhD, a former Stanford Biodesign fellow, and his new company are testing two tiny devices that stimulate natural tear production by delivering micro-electrical pulses to the lacrimal gland. One model is inserted into the mucous membrane in the nasal cavity, and the other is inserted under the skin below the eyebrow. Tear delivery rates can be adjusted manually with a wireless controller.
Stanford Biodesign is a training program in medical-technology innovation and development. Each year, it admits 12 applicants with backgrounds in medicine, engineering and business. These Biodesign fellows work to address unmet medical needs through the development of new technologies and devices.
Ackermann, 32, who has a boyish grin and buzz-cut hair, joined the program in 2010 after earning a PhD in biomedical engineering from Case Western Reserve University and working on chronic-pain and movement-disorder devices at Boston Scientific, a medical device corporation. He said he enjoyed the corporate work but realized he wasn’t a big-company person.
“I thought the Biodesign Program was a good opportunity to try out entrepreneurship in a safe, academic environment,” he said.
Solving problems with fresh eyes
At the start of the program, Ackermann was assigned to a four-person team tasked with looking for medical needs in eye clinics. His team members included Victor McCray, MD, a board-certified surgeon; Brandon Felkins, a graduate student in mechanical engineering at California Polytechnic State University-San Luis Obispo; and Garrett Smith, a PhD candidate in bioengineering at UC-San Diego.

Michael Ackermann
They began by observing all facets of a busy ophthalmology practice, shadowing the doctors and interviewing them and their patients. At the end of two months, they had documented more than 300 clinical needs.
Early in this process, Ackermann recognized dry eye as a promising area. “Every third person visiting the clinic seemed to be suffering from dry eye, which ranged from something that was a nuisance to a genuine, sight-threatening disease,” he said. “It was a huge medical need with no optimal treatments.”
With every blink, healthy eyes are lubricated with tears — a mixture of oils, water, proteins and mucus. This fluid helps protect and moisturize the eyes, and the thin film that it creates is necessary for clear vision. Dry eyes become vulnerable to painful abrasions of the cornea, which can distort vision.
Dry eye can be triggered by a number of factors, including gland defects, medication side effects and hormonal changes caused by pregnancy or menopause. It is also associated with some immune-system disorders.
“There are very poor treatment options for my dry-eye patients,” said Mark Blumenkranz, MD, professor and chair of ophthalmology, who was a mentor for the fellows on this project.
The two most common dry-eye treatments are lubricating eyedrops and cyclosporine, a topical emulsion, but both have drawbacks. The eyedrops require refrigeration, making them difficult to apply when needed, and they don’t replicate all the vital components of natural tears. The topical ointment treats the inflammation associated with dry eye but not the root cause of the condition.
There are very poor treatment options for my dry eye patients.
“We’ve observed that more than half of our dry-eye patients stop taking cyclosporine after a few months,” Blumenkranz said. “This high dropout rate led the team to believe that patients and physicians would be open to new treatment options.”
Paul Yock, MD, director of Stanford Biodesign, said, “The key to biomedical technology innovation is getting the need right. Michael and his team appreciated that dry eye was a latent need, in that these patients were being inadequately treated, with no real breakthroughs in years. In this kind of situation, the need quietly recedes into the background, as patients and providers become complacent with the status quo.”
Aiming for a market blind spot
Once the fellows focused on dry eye, they spent the next few months coming up with hundreds of treatment ideas. Then, they systematically analyzed each for technical feasibility, the ability to fit into a physician’s workflow and the potential to generate revenues. During this phase, the Biodesign community — faculty mentors, working physicians and venture capitalists — provided invaluable feedback, Ackermann said.
“Because of my background in neuromodulation, I wondered if we could stimulate the nerves in the lacrimal gland to generate tears,” Ackermann said.
It was a radically different idea, but after conducting extensive research, they thought this concept was worth a try. But their first product configuration was poorly received by clinicians.
“Initially, we envisioned a large implanted device with a wire coming up inside the neck, similar to a pacemaker,” said Ackermann. “We took it to eye specialists, who said, ‘That is never going to happen.’”
So they went back to the drawing board and built several versions of a much smaller model out of plastic and clay. They took these prototypes back to the eye specialists, who thought the devices, when actually made, could be injected under the eyebrow with a large-gauge needle in a doctor’s office.
“At first, I thought their solution was quirky,” Blumenkranz said. “But nobody was thinking about the neurological basis of dry eye. I recognized that it had the potential to be a breakthrough product.”
Building the business
Between March and June of 2011, the team entered its business plan into a number of startup competitions. The team placed in six of them, earning more than $32,000 in prizes and thousands more in business-development services. This was enough to fund a prototype effort.
As the fellowship year came to a close, Ackermann was accepted as a second-year Biodesign fellow. During that year, he decided to launch a company, called Oculeve, to develop tear-stimulation devices and bring them to market. For help with the technical challenges, he teamed up with Daniel Palanker, PhD, professor of ophthalmology at Stanford, and Jim Loudin, PhD, a postdoctoral scholar in Palanker’s lab and an expert in stimulator design who is now Oculeve’s vice president of research and development.
McCray and Felkins decided to launch another startup, Ocular Dynamics, which is developing a fluid that helps prevent the drying of contact lenses. Smith went on to earn a PhD and is now co-founder and chief technology officer of Nasseo, a startup developing a novel dental implant technology.
Oculeve caught the attention of Brook Byers, a founding member of the distinguished Silicon Valley venture-capital firm Kleiner Perkins Caufield & Byers. “Oculeve was after a large market with weak competition,” Byers said. “They had a clever new invention, a good economic model and a strong starting team.”
Byers then convinced the firm to commit $100,000 in seed funding, and this enabled Oculeve to test a prototype for efficacy and safety in animals.
The first time I saw our device actually working in a real patient, it was out of this world.
In October 2012, after proof-of-concept testing, Byers and Ackermann assembled a group of health-care venture capitalists — KPCB, Versant Ventures and New Enterprise Associates — and convinced them to invest $7.6 million into the startup. With this funding, they were able to hire much-needed employees and launch clinical trials in Australia, New Zealand and Mexico.
“The first time I saw our device actually working in a real patient, it was out of this world,” Ackermann said.
In May 2014, Oculeve investors contributed an additional $16.6 million to the company. That money will hopefully carry the company through the expensive, time-consuming process of getting a medical device through its European and Canadian round of regulatory approvals, Ackermann said. U.S. regulatory approvals are in progress, and patients interested in participating in future clinical trials can visit http://www.clinicaltrials.gov (and search for “Oculeve”).
Today, Ackermann runs his 20-person company from a corner office with a panoramic view of the San Francisco Bay. When asked about the challenges of launching a company, Ackermann points to a quarter-sized patch of gray hair on the crown of this head: “This wasn’t here before I started. It’s incredibly hard managing a company where the money only flows out. I won’t consider it a success until the products are on the market, treating patients and profitable.”
And when this happens, there probably won’t be a dry eye in the house.
Early support for this project came from Biodesign, which is part of the university’s interdisciplinary Bio-X institute; and Spectrum, the Stanford Center for Clinical and Translational Research and Education.
Blumenkranz sits on the board of Oculeve.
-
 Kris NewbyKris Newby is the communications manager for Spectrum, the Stanford Center for Clinical and Translational Research and Education. Email her at krisn@stanford.edu.
Kris NewbyKris Newby is the communications manager for Spectrum, the Stanford Center for Clinical and Translational Research and Education. Email her at krisn@stanford.edu.
About Stanford Medicine
Stanford Medicine is an integrated academic health system comprising the Stanford School of Medicine and adult and pediatric health care delivery systems. Together, they harness the full potential of biomedicine through collaborative research, education and clinical care for patients. For more information, please visit med.stanford.edu.

