Umbilical Cord

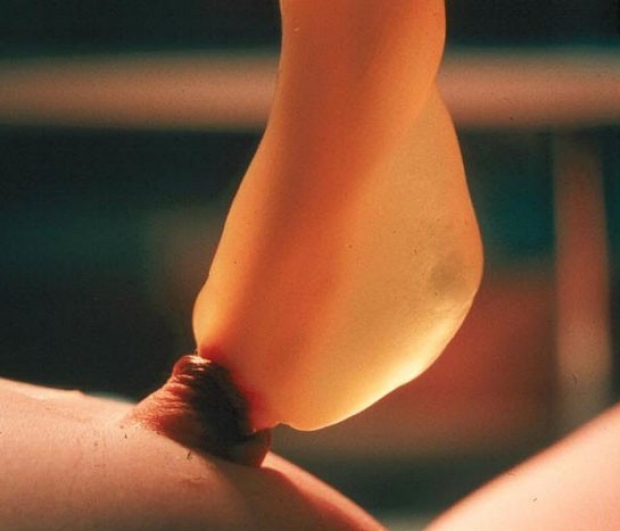
Normal Umbilical Cord
This infant is 7 hours old. The cord is plump and pale yellow in appearance. One of the umbilical arteries is visible protruding from the cut edge. A normal cord has two arteries (small, round vessels with thick walls) and one vein (a wide, thin-walled vessel that usually looks flat after clamping).
photo by Janelle Aby, MD

Normal Umbilical Cord
Looking at the cut edge more clearly shows the normal vessels of the umbilical cord. The two arteries are to the left and the vein, with a spot of blood in its large lumen, is on the right.
photo by Janelle Aby, MD

Normal Umbilical Cord
The dark stripes within the cord in this picture are examples of intravascular clots -- a normal finding in newborns. In some cases, the vessels are so full of clotted blood that all three may be clearly identified as they wind around through the umbilical stump.
photo by Janelle Aby, MD

Normal Umbilical Cord
This infant is 19 hours old. The cord is beginning to dry and darken as it makes its transition into a non-functioning organ.
photo by Janelle Aby, MD

Normal Umbilical Cord
After a couple of days, the cord is a stiff, dry stump. The bulge of skin around the edge is a normal variant and does not represent an abnormality.
photo by Janelle Aby, MD

Normal Umbilical Cord
Just minutes after the cord falls off, some of the remaining moist debris is still visible on the skin. A spot of blood or a slight amount of moist, yellow material may be present on the diaper or clothing after cord separation. Any bleeding or discharge that persists should be evauated, as this is not a normal finding.
photo by Janelle Aby, MD