General
-
Appropriate for Gestational Age
-
Small for Gestational Age
-
Large for Gestational Age
-
Discordant Size
-
Acrocyanosis
-
Perioral Cyanosis
-
Facial Bruising
-
Meconium Staining
-
Meconium Stained Umbilical Cord
-
Meconium Stained Vernix
-
Jaundice
-
Colostrum
-
Bilious Emesis
-
Mature Milk
-
Green Breastmilk
-
Digested Blood
-
Meconium
-
Transitional Stool
-
Yellow Stool
-
Normal Stool
-
Meconium Plug
-
Normal Urine
-
Urate Crystals
-
Normal Vaginal Blood

Appropriate for Gestational Age
One of the earliest observations an examiner can make when evaluating a newborn is that of size. Because small term babies and large preterm babies may be the same weight but have very different problems, the categorization of size should always be made in relationship to the gestational age. Babies who are large or small for their age need special consideration. Typically, term babies are appropriate for gestational age (AGA) when their weights fall between 5lb 12oz (2.5kg ) and 8lb 12 oz (4kg). This baby, at about 7 pounds is AGA.
photo by Jim Bryson

Small for Gestational Age
Because they have decreased glycogen and fat stores, small for gestational age (SGA) babies are particularly prone to hypoglycemia after birth; routine glucose measurements during the first few hours of life are recommended. Polycythemia is also common, and is related to the increased erythropoetin levels produced by a relatively hypoxic uterine environment. Fetal growth is influenced by many factors, but decreased uteroplacental function related to pregnancy induced hypertension (PIH) is a fairly common etiology. This baby was mildly SGA with a birth weight of about 5 1/2 pounds. Relatively thin extremities and torso give this baby a typical SGA appearance.
photo by Janelle Aby, MD

Large for Gestational Age
In contrast, this infant is large for gestational age (LGA) with a birth weight of about 9 1/2 pounds. These infants have much more glycogen at birth, but hypoglycemia may still be a problem as many of these babies are infants of diabetic mothers. When the ample glucose supply is interrupted with the cutting of the umbilical cord, the babies' pancreas may take a while to down-regulate, leaving the infant with high insulin and low glucose levels in the meantime. Polycythemia may also be present. The plump extremities, torso and full cheeks of this infant (though mild in this photo) are typical features of an LGA baby.
photo by Janelle Aby, MD

Discordant Size
When it comes to evaluating multiples, comparison of size between individuals is also important. Discordance between siblings may indicate placental inequalities, twin-twin transfusion syndrome, or other problems. These twins differ in weight by about 1 pound (0.5kg); the smaller twin, on the bottom in this photo, weighed 5 pounds and the larger one was over 6 pounds. Hematocrits were checked on both (a routine in our nursery for twins of any size) and were normal. The infants were otherwise healthy and did well.
photo by Janelle Aby, MD

Acrocyanosis
Shortly after birth, cyanosis of the hands, feet, and perioral area are common findings. In this photo, notice the difference between the color in the feet and the color of the legs and abdomen. Acrocyanosis typically resolves in 24 - 48 hours.
photo by Janelle Aby, MD

Acrocyanosis
Another view of the same infant. Note the contrast between the feet and the color of the right leg.
photo by Janelle Aby, MD

Acrocyanosis
As this infant is transitioning, the blue color on the feet is starting to resolve over the upper part of the sole, but is still clearly present in the toes and, to a lesser degree, on the rest of the sole.
photo by Janelle Aby, MD

Acrocyanosis
Here again, the cyanosis of the feet is apparent in comparison to the parent's hand and the baby's chin in the background.
photo by Janelle Aby, MD

Perioral Cyanosis
A blue color around the lips and philtrum is a relatively common finding shortly after birth. This is part of acrocyanosis. The skin in this infant is visibly well perfused, and the tongue and mucous membranes in the mouth were pink, a finding that assures the examiner that central cyanosis is not present. This finding resolved spontaneously over the next 48 hours.
photo by Janelle Aby, MD

Perioral Cyanosis
Another newborn with perioral cyanosis clearly demonstrates that although the philtrum and upper chin have a dark tint, the lips and tongue are bright pink.
photo by Jim Bryson

Facial Bruising
Marked bruising of the face can occur during delivery. It is more common when there is a tight nuchal cord, when the delivery is precipitous or difficult, or when the infant is large. When the infant is bundled, this facial appearance could be mistaken for cyanosis, but with a quick comparison to the color of the rest of the body, the diagnosis is obvious. This type of bruising resolves over the course of several days.
photo by Janelle Aby, MD

Facial Bruising
This is another example of facial bruising. Here again the face appears to be cyanotic (including the lips), but the tongue and the rest of the body had a normal pink color. On careful examination, petechiae where also noted across the forehead. This is another manifestation of bruising in a newborn; no further evaluation is needed.
photo by Janelle Aby, MD

Meconium Staining
Evidence of meconium staining in utero may be a clue to an infant who was stressed before birth. In this picture, meconium staining can be appreciated on the fingernails. Normally, the nails are white. The yellow tint is meconium staining. This suggests that the meconium was present in utero for some time prior to delivery. Staining may also be seen on the umbilical cord and the skin.
photo by Janelle Aby, MD

Meconium Stained Umbilical Cord
This cord is about 7 hours old at the time of the photo, but the normal light yellow color is not visible, even though the cord is still plump. It is the presence of meconium in the amniotic fluid which gives it a dark green color. Although meconium staining has no direct effect on the infant, the presence of meconium is often associated with in utero stress.
photo by Janelle Aby, MD

Meconium Staining
In this infant, it is not the skin itself, but the vernix that shows evidence of meconium in the amniotic fluid. Vernix caseosa is the pasty, cheese-like, material present in varying degrees on the skin at birth (here a small amount of vernix is seen on the back shortly after delivery). It is a mixture of sebum produced by the infant's skin and cellular debris that has accumulated in utero. Normally, vernix is a creamy white color. The yellowish brown tint seen in this photo is a result of meconium staining.
photo by Janelle Aby, MD

Jaundice
When assessing jaundice comparisons are useful. Since the type of lighting in a room can dramatically affect the appearance of the skin, comparing the infant's color to the parents' color, or comparing the facial color of the infant to the color of the infant's feet can highlight differences. If one is just looking at the face of this infant, the yellow tint might be thought to be the baby's skin tone. Here the hand provides a nice contrast -- the undertones there are much whiter.
photo by Janelle Aby, MD

Jaundice
In this picture, the cephalo-caudal progression of jaundice in the newborn can be seen. If one were describing jaundice in this infant, "jaundice to the chest" would be useful. Although repeated studies have shown that accurate prediction of bilirubin levels is not possible by exam, even with an experienced examiner, terms that assess the intensity and body area visually affected are meaningful when trying to determine whether the jaundice is progressing or improving over time.
photo provided by parents

Jaundice
Here, the jaundice is much more intense. Notice again the contrast between the fathers' hand color and the baby's face. The bilirubin level in this infant was approximately 20 mg/dL.
photo provided by parents

Jaundice
It is important for the examiner to understand that babies who are undergoing phototherapy treatment have an unreliable skin exam due to the temporary "bleaching" effect of phototherapy on exposed skin. Here, minutes after the baby is removed from under the bili lights, a clear color demarcation can be seen between the skin that was under the eye cover and the skin that was exposed to the lights. Serum bilirubins are the only useful measure of progress with phototherapy.
photo by Janelle Aby, MD

Colostrum
Colostrum, which is the breast milk produced during the last part of pregnancy and the first few days after the birth of the baby, differs from mature milk in appearance, nutritional content, and volume. Although a typical feeding of colostrum is only a teaspoon (5ml) or less, it contains a large amount of protective immunoglobins that give the baby his/her first protection against infection. It is much more yellow in appearance than mature milk and has a thick, sticky consistency.
photo by Jane Morton, MD

Colostrum
This colostrum was spit up by a newborn shortly after a feeding. Again the bright yellow color and sticky consistency can be appreciated. For some mothers, colostrum can appear almost neon in color. It is important not to confuse spit-up colostrum with bilious emesis, which would be more green and would not occur in a well newborn.
photo by Janelle Aby, MD

Bilious Emesis
For comparison, this is an example of bilious emesis. The green color of bile is clearly present here. This newborn was thought to be well and was tolerating feedings for several days before the sudden onset of this abnormal emesis. Malrotation with volvulus was diagnosed and the infant underwent emergent surgical correction. Emesis like this is never normal.
photo by Janelle Aby, MD

Mature Milk
Once the milk "comes in" and the volume increases significantly (usually around the third post-partum day), the milk changes in appearance from the yellow, sticky colostrum to the more creamy, liquid mature milk. The exact appearance, though, changes even within a feeding. The milk expressed at the beginning of the feed will have a lower fat content (and appears thinner) than the milk expressed as the breast is progressively emptied. The later "hindmilk" has a high fat content and looks thicker and creamier.
photo by Janelle Aby, MD
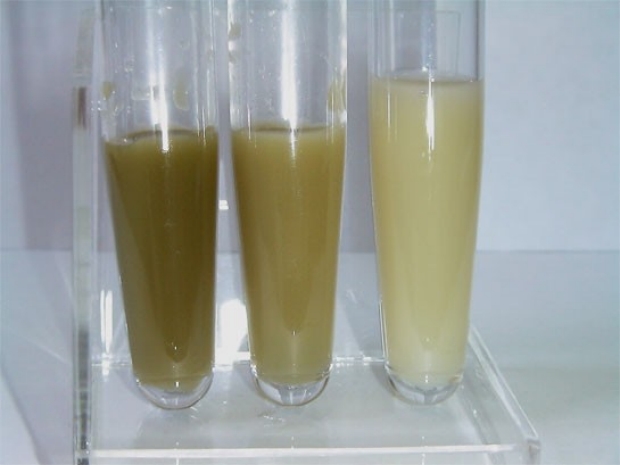
Green Breastmilk
At times, human milk comes in surprising colors. These samples of milk were obtained from the same mother on day 2, day 3, and day 4 post delivery (left to right). The greenish tint has several possible etiologies, none of which are dangerous to the newborn. During the marked proliferation of lactiferous tissue during early lactation, some red blood cells may leak into the milk from the mothers' circulation and create discoloration (rusty pipe syndrome), a likely cause of the discoloration in this case. Spontaneous resolution is expected in several days. In the photo above, clearing of the milk has already occurred by day 4. Other suspected causes of green milk include seaweed (especially when ingested in tablet form), green-colored sports drinks, herbal vitamins, and iron tablets.
photo by Dr. Jorge Colomer, Hospital de la Plana, Castellón Valencia, Spain

Digested Blood
During the process of delivery, a newborn will occasionally swallow small amounts of maternal blood. When this is spit back up after delivery (usually during the first 24 hours), it typically causes some anxiety for caregivers. The appearance above, where the blood appears to be partially digested, is common, but bright red blood can also be of maternal origin. In an otherwise well newborn, close observation is the only necessary intervention. If doubt exists about the origin of the blood, an Apt test can be performed on the sample.
photo by Janelle Aby, MD

Digested Blood
This is another example of regurgitated blood, likely of maternal origin.
photo by Janelle Aby, MD

Meconium
Meconium stools are characterized by their dark (almost black) color, sticky consistency and odorless nature. Normal passage of meconium should include at least one stool in the first 48 hours after birth and end with the onset of transitional stools by day 4. Delayed passage of meconium should prompt consideration of Hirshsrung's disease or conditions associated with meconium plugs. Delayed conversion to transitional stools should prompt evaluation of feeding adequacy.
photo by Janelle Aby, MD

Transitional Stool
Transitional stool represents the change from meconium to the normal yellow, seedy stools that characterize infants feeding on milk only. Here, the dark color of meconium is still visible, but lighter, yellowish curds can also be seen. Exclusively breastfed infants should have transitional stools by day 4 if feedings are adequate.
photo by Janelle Aby, MD

Yellow Stool
This is the normal appearance of stool in an infant who is excusively breastfed. This appearance is typically described as "bright yellow and seedy". Note there is a significant amount of liquid stool absorbed into the diaper with only some solid material on top. This is sometimes thought to be diarrhea by parents, but it is not. The presence of this type of stool by day 5 is a reassuring sign that the infant is being well fed.
photo by Jane Morton, MD

This is the stool of a 2 week old infant who was being fed an extensively hydrolyzed formula. The stool is normal, but has less of the bright yellow, seedy consistency of a breast-fed infant stool.
photo by Janelle Aby, MD

Meconium Plug
Here is an example of a stool that is not normal. This is a meconium plug. It is a very viscous, congealed mass of meconium that may either be spontaneously passed or may create an obstruction and be the cause of delayed stooling. Typically, after the infant passes the plug, the subsequent stool is normal. Although there is a known association between an underlying diagnosis of cystic fibrosis (CF) and meconium plug, many infants with this finding do not have CF. The majority of cases are thought to be caused by an immaturity of the ganglion cells of the colon, leading to a transient impairment of colonic function. Maternal diabetes and prematurity are known risk factors.
photo by Janelle Aby, MD

Normal Urine
Normal urine soaked into a diaper. Because of the absorbency of disposable diapers, the surface will not feel wet, even with this considerable amount of urine. If knowing output is important, dry and wet weights of the diaper can be measured.
photo by Janelle Aby, MD

Urate Crystals
Often mistaken for blood in the urine, urate crystals are a frequent intermittent finding in the first week. The characteristic appearance of pink-orange material is sufficient to make the diagnosis. No laboratory analysis is needed.
photo by Janelle Aby, MD

Urate Crystals
Another example of urate crystals in a diaper. Even in the urine-soaked areas, a pink tinge is visible.
photo by Janelle Aby, MD

Normal Vaginal Blood
This is normal vaginal withdrawal bleeding that occurs in some female infants. Similar to withdrawal bleeding in adolescents, this typically occurs on the third day after birth, continues for a few days, then stops.
photo by Janelle Aby, MD

Normal Vaginal Blood
Here is another example of normal vaginal withdrawl bleeding in a newborn girl. For the first 3 days, no blood was noted. This photo was taken of a diaper produced on day 4. On physical exam, blood could be seen in the vaginal area, but was otherwise normal. Bleeding may be noted in every diaper for a couple of days, but will spontaneously resolve. Large amounts of blood are not normal for withdrawl bleeding. If bleeding seems excessive, vitamin K deficient bleeding or other coagulopathy should be considered.
photo by Janelle Aby, MD