Bronchoscopy
What Is a Bronchoscopy?
By Carol Conrad, MD, Stanford CF Center
Your doctor may advise you that your child should undergo a procedure called a bronchoscopy. A bronchoscopy is a procedure that allows us to look at the airways, or the tracheobronchial tree, through a special sort of “scope”, called a bronchoscope. With the bronchoscope, we can evaluate the respiratory system, including the voice box (larynx), the wind pipe (trachea), and the airways (bronchi) for evidence of any abnormality or infection.
Why is a bronchoscopy done?
Sometimes it is important to watch the movement of these structures during the different stages of the breathing cycle. At times it is important for diagnostic purposes to obtain some of the fluids in the lung through the bronchoscope for evaluation in the laboratory. The scope has a special channel through which we can vacuum some of the liquid lining from the airways. A bronchoscopy allows a physician to perform diagnostic tests, to obtain specimens for biopsy and culture, or to remove foreign objects that children might have inhaled.
What is a bronchoscope?
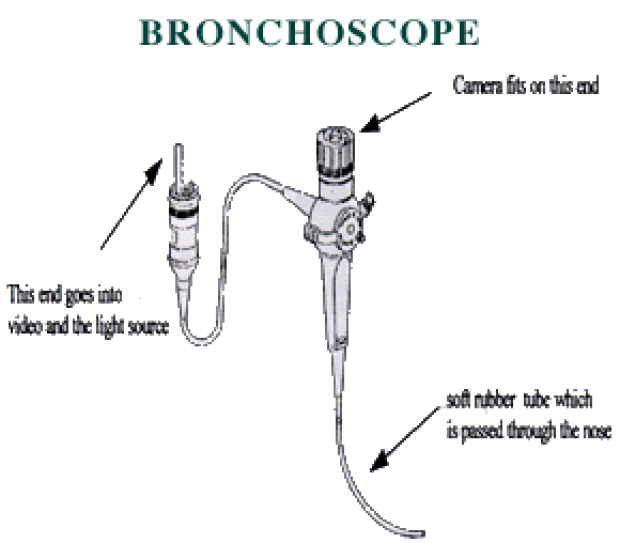
The bronchoscope is a soft (flexible) tube with an outer diameter as small as 2.2 mm and there are larger sizes for use with larger children and adults. The scope can be easily passed through the nose or the mouth. The flexible tube actually contains a fiber-optic system which attaches to a video camera and a source of light. The light travels through the scope and lights up the inside of the airway. The image seen at the tip of the scope is transmitted back again through the fiber-optic system to the video camera. We can also take photographs through the scope.
What information do you get from a bronchoscopy?
A bronchoscopy enables the physician to see and test the material that is deep in a patient's lungs. Sometimes bacteria lodge deep in the lungs, and it can be difficult to find or identify them. This material can be washed out by washing the airways with saline. This is referred to as a bronchoalveolar lavage (BAL). The physician injects a small amount of saline through the bronchoscope into the airways and then sucks it back through the suction port of the bronchoscope. The fluid obtained contains saline plus secretions from the lung: bacteria (if present), cells, etc. This sample is sent to the laboratory for testing.
How is a bronchoscopy done?
A bronchoscopy is done in a special room in the outpatient ambulatory procedure unit at the Packard Children's Hospital. Typically, a bronchoscopy is performed with the patient sleeping, but breathing on their own. The patient is given medications to produce sedation (a sleepy state). At times, biopsies, or very small pieces are obtained from the lungs, and this may require the use of general anesthesia, but most bronchoscopies are done under sedation. The patient is arousable from this sleep and is able to cough, sneeze, or may try to speak if directed. We keep a close watch on the patients with monitors that continuously check the patient's vital signs such as heart rate, blood pressure, and blood oxygen levels (oximetry).
After the patient is asleep, the next step is to numb the nose and back of the throat. Numbing drops (Lidocaine) are sprayed into the nose. Later on during the procedure, this medicine can be applied to the airways though the bronchoscope to numb other structures such as the larynx, trachea, and bronchi as they are encountered. The Lidocaine prevents irritation from the scope to the airways, and can minimize coughing and sneezes. After the numbing medicine is applied, the bronchoscope is inserted through one nostril, and the procedure begins.
How long will this take?
The patient usually comes to the outpatient surgical center an hour or so before the scheduled bronchoscopy begins. This allows time to fill out insurance and medical forms, and in the pre-operative unit, vital signs are recorded, and a brief physical exam is done. At about this time, an IV line is placed by the nurses. The actual bronchoscopy takes about 45 minutes. After the procedure is done, the patient recovers in the post-anesthesia care unit until he/she is awake and is able to go home. The medicines used for sedation are considered to be “short-acting”, but parents often report that the baby sleeps through much of the rest of the day. The entire procedure takes about 4 hours in the hospital.
What are the risks of the procedure?
Flexible fiberoptic bronchoscopy is generally very well-tolerated and safe, even in very young infants. However, there are certain complications that are associated with flexible bronchoscopy. The most common problem is a fever that occurs after the procedure. This is usually a low grade fever (rarely over 101°) and usually responds to acetaminophen (Tylenol, Tempra, or other brands). Your child may experience some mild bleeding from the nose. This responds to pressure and is rarely encountered in children who are not predisposed to bleeding problems. In patients who are having a biopsy performed, a pneumothorax is a concern. This results in the collection of air around the lung and may result in collapse of a lung. A tube may need to be placed to evacuate the air and allow the lung to re-expand. Your child may require supplemental oxygen during and after the procedure. If he/she is having respiratory difficulties, we may need to place a temporary breathing tube in your child's airway and breathe for him or her. Finally, oversedation may necessitate a longer recovery period for your child and in rare instances, an overnight hospitalization.