Approach
In our studies, we use a combination of intracranial electroencephalography (iEEG), functional MRI (fMRI), and intracranial electrical stimulation (iES). Here we explain each method very briefly:
Intracranial EEG (iEEG)
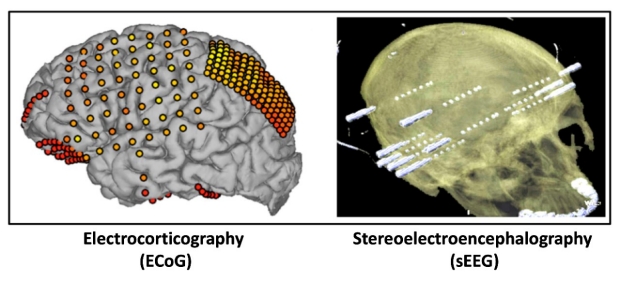
When EEG recordings are obtained with intracranial electrodes, we refer to it as intracranial EEG (iEEG). If strips or grids of electrodes are implanted over the bare cortex in the subdural space, we use the term electrocorticography (ECoG). If electrodes are inserted as thin wires of intracranial electrodes through small burr holes in pre-defined stereotactic coordinates of the brain without opening the skull bone, we refer to it as stereotaxic-EEG or simply stereo-EEG (sEEG).
Human iEEG can complement other methods of neuroscience beyond simply replicating what is already known, or can be known, from noninvasive lines of research in humans or from invasive recordings in nonhuman mammalian brains. For more information see: Parvizi J, Kastner S. Promises and limitations of human intracranial electroencephalography. Nature Neuroscience. 2018
Functional MRI or fMRI
This is an MRI scan of the brain that reveals where the brain is more activated or less activated during a task. If it is done during rest, it is called resting state fMRI or rs-fMRI to reveal which regions of the brain have synchronous fluctuation of activity (hence they might be working in unison and may be part of a so-called “resting state or intrinsic functional network”).
In each patient before surgical procedure, we obtain task or resting state fMRI. After the electrodes are placed, we can superimpose their location on the fMRI space and identify electrodes that are located in a specific functional region or in a specific intrinsic resting state network.
In this figure you see location of electrodes in the resting state fMRI space. Each color denotes a specific resting state network.

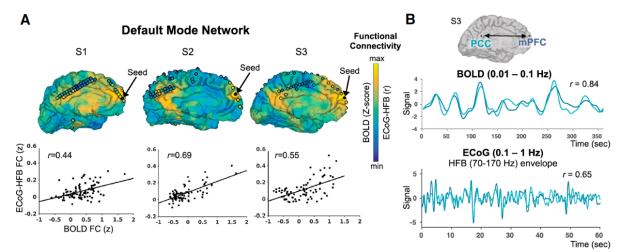
We have confirmed correspondence between resting state BOLD and iEEG seed-based functional connectivity maps within subjects. The figure below shows individual results from 3 participants with seed locations within the mPFC. Note how specific electrodes in the posterior cingulate are connected with the mPFC seed and how their location corresponds with a larger BOLD connectivity (see Kucyi et al. Journal of Neuroscience 2018)
We have also confirmed that the signature of iEEG, in some instances, follows the map of resting state networks (see the iEEG responses in the frontoparietal (blue) and dorsal attention (green) networks that were identified by the same individual’s pre-operative ds-fMRI.

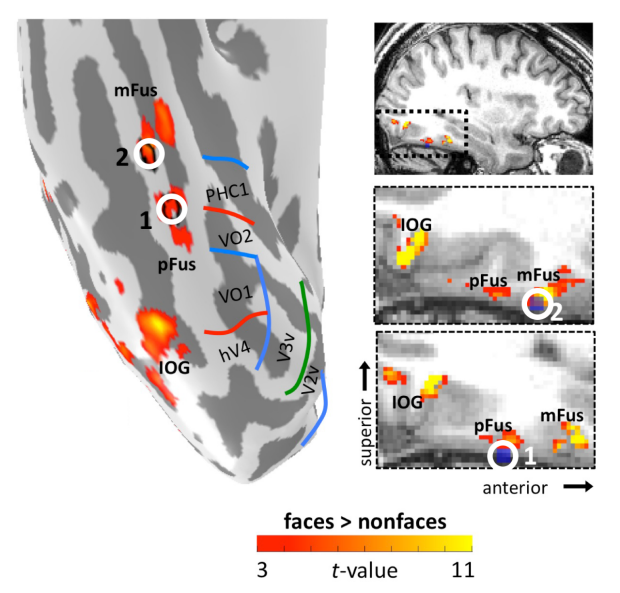
As another example, you see here how a patient’s two electrodes (1 and 2) are located exactly at the center of fMRI defined region of the brain that is specialized in processing faces.
Intracranial Electrical Stimulation (iES)
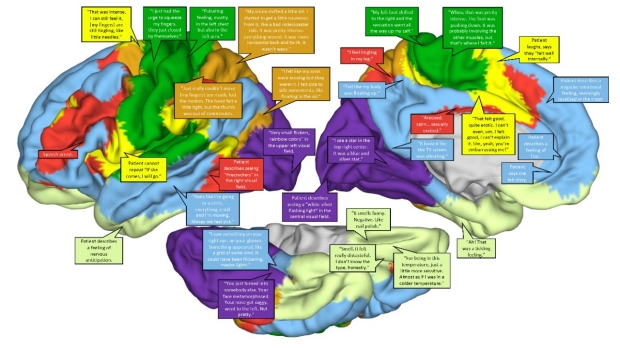
Direct electrical stimulation of the brain provides unique insights about the causal importance of a given brain region and its anatomical network in a specific set of functions. During this procedure, we inject electrical current through implanted electrodes when the patient is either relaxing or doing an experiment. We probe how their subjective state changes with real or sham electrical stimulations or how their performance in a given experiment is altered due to electrical perturbation of neurons in a given region of their brain.
In a series of experiments, we have probed the causal importance of specific brain areas (and their interconnected networks) in specific functions.
Reference: Fox KCR, Shi L, Baek S, Raccah O, Foster BL, Saha S, Margulies DS, Kucyi A, Parvizi J. Intrinsic network architecture predicts the effects elicited by intracranial electrical stimulation of the human brain. Nature Human Behaviour. 2020. Epub 2020/07/08. doi: 10.1038/s41562-020-0910-1. PubMed PMID: 32632334.
Example:
Reference:
Parvizi J, Jacques C, Foster BL, Witthoft N, Rangarajan V, Weiner KS, Grill-Spector K. Electrical stimulation of human fusiform face-selective regions distorts face perception. J Neurosci. 2012;32(43):14915-20. Epub 2012/10/27. doi: 10.1523/JNEUROSCI.2609-12.2012. PubMed PMID: 23100414; PMCID: PMC3517886.
Reference:
Schrouff J, Raccah O, Baek S, Rangarajan V, Salehi S, Mourao-Miranda J, Helili Z, Daitch AL, Parvizi J. Fast temporal dynamics and causal relevance of face processing in the human temporal cortex. Nature communications. 2020;11(1):656. Epub 2020/02/02. doi: 10.1038/s41467-020-14432-8. PubMed PMID: 32005819; PMCID: PMC6994602.
We can also use iES method to inject repeated pulses of electricity in a specific area of the brain while recording from all other regions. By examining the presence, and the mode, of evoked responses in the recorded areas we can examine the details of connectivity across the stimulated and recorded areas.
Pairs of electrodes stimulated and evoked potentials recorded from each other pair of electrodes are shown here. Also shown is an example of a bipolar stimulation from a depth electrode depicting the typical deviation from baseline activity over time.

Our research is performed in clinical settings and in patients with medication-resistant epilepsies. We actively minimize the confounding effect of epilepsy on the acquired data by the following measures: 1) we exclude patients with diffuse brain disease; 2) we exclude electrodes with epileptiform discharges (more than 80% of recording sites are usually void of epileptic activity); 3) we exclude trials coinciding with epileptic discharges; 4) we obtain data several hours outside the window of seizures; and most importantly, 5) we confirm that findings are anatomically and functionally consistent across a number of patients - each with different source and type of seizures. When possible, we also show that findings in our clinical population are akin to findings reported in non-invasive studies of healthy subjects. Recently, we confirmed that non-lesional epileptic tissue has normal physiological responses to relevant cognitive stimuli, but their responses are “seized” by ongoing spontaneous epileptic activity in a window of -1050ms to +200ms around the stimulus onset. Liu S, Parvizi J. Cognitive refractory state caused by spontaneous epileptic high frequency oscillations in the human brain. Science Translational Medicine. 2019