Interventions
Introduction
Before you determine what interventions may be relevant for your children or adolescents with sleep challenges, you should assess what are the problems. Please see Figure 10 below for the five categories of common sleep problems:

Figure 7. Assessing sleep problems in children and adolsecents on the autism spectrum.
A. Non-pharmacological Interventions
In general, common sleep problems children and adolescents on the autism spectrum face involve resistance to go to sleep and sensory issues. Some cannot sleep well because of anxiety or other sleep conditions, such as sleep terror. Please see below for some behavioral strategies that may be used for these sleep problems. Routine and environment are important factors in sleep. Keeping a sleep journal can help your healthcare provider identify potential thoughts, routines, or behaviors that may be helping or hurting your sleep quality. Like any behavioral intervention, consistency is the key. You will need to make sure others in the household are all consistent with the changes associated with the intervention. After you have tried the strategies and are still not satisfied with the outcome, then you may want to seek consultation from your healthcare providers.
Sleep Hygiene
Healthy habits, behaviors, and environmental factors that can be adjusted to help you have a good night's sleep. For children on the autism spectrum, sleep hygiene practices may need to be adapted to fit the unique needs of the child and family.

Basic Principles include:
• Choosing an appropriate bedtime
• Consistent sleep and wake times
• Creating a predictable routine
A predictable bedtime routine might include a wind-down activity such as a bedtime story or listening to music, taking a warm shower, wearing the same pajamas, or using a visual prompt/sequence to communicate that you are transitioning to bedtime.
• Minimizing screen time before bed [19]
• Blue light blocker glasses.
• For children who use screen technology to communicate or self-regulate, apps that remove high blue light.
Figure 8. Basics of sleep hygiene.
Reducing stimulation before bed
• Limit foods/beverages containing caffeine in the evening.
• Avoid emotionally stimulating activities such as playing outside or watching exciting TV.
Creating a good sleep environment
• Consider the temperature of the room (preferences can vary widely), the textures of bedding and sleep clothes (look for materials that your child likes or that don’t cause sensory issues), light levels (blackout curtains or night light), noise levels (music or white noise), pressure on the body (weighted blankets) and visual stimuli in the room.
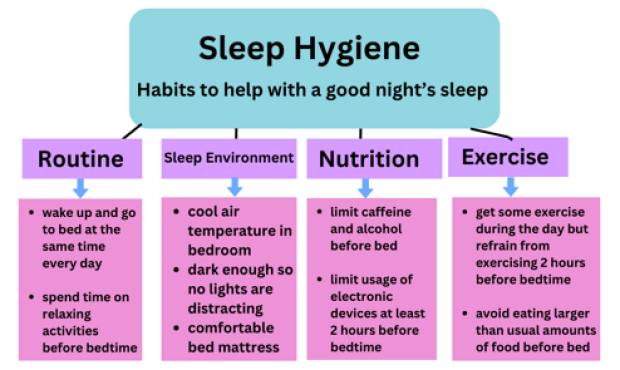
Figure 9. Sleep Hygiene Tips [13]

Strategies to manage resistance to sleep:
Cueing
• Cueing uses components of modeling, visual supports, sticker charts, and social stories to promote positive bedtime habits.
Positive reinforcements
• Morning rewards (e.g., wrapped presents from a dollar store or a warm blanket from the dryer) can reinforce positive sleep habits.
Strategies to manage sensory issues:
Compression Bed Sheets
• Compared to weighted blankets, compression bed sheets are less constrictive and more breathable. These sheets provide adjustable pressure and sensory support, helping individuals with autism to sleep better. They are made of breathable and stretchy materials, such as lycra, nylon, and spandex, and are available in different sizes to fit various mattresses.
Weighted Blankets
In children on the autism spectrum, the use of a weighted blanket did not result in improvements in duration of sleep, sleep onset, or awakenings. However, the weighted blanket was favored by children and parents, and blankets were well tolerated over this period. [20]
STS Mattress Technology
Recent studies find STS mattress technology well-tolerated and reported as easy-to-use by parents of autistic children. Parent diary outcomes recorded better quality sleep and daytime behavior [21].
Figure 10. Tips for keeping sleep journals effectively.
Strategies to manage anxiety issues:
Massage
Massage can impact sleep quality by reducing anxiety and physical discomfort. The process increases circulation, supports the immune system, and releases muscle tension. Physical relaxation and quieting the mind can make it easier to fall asleep. [22]
Strategy to manage night terrors:
Scheduled Awakenings
Scheduled awakening requires the child to be woken before the time that they usually experience an episode of sleep terror-induced night waking to alleviate night terrors. Awakenings should gradually be diminished.
Helpful for children with lots of energy before going to bed:
Exercise
Try encouraging your child to be active in a way that works for them. This should be done during the daytime and not the last hour before going to bed. Exercise doesn’t have to mean playing sports or working out, although these are both good options. Walking, dancing, jumping, spinning, or swimming are also great ways to exercise. [23]
Strategy to wean co-sleeping:
Stimulus Fading
Stimulus fading is a method that specifically targets co-sleeping (when the child has difficulty falling asleep without the caregiver in the bed/room); stimulus fading involves the gradual distancing of the parent from the child’s bed until the child is able to fall asleep without them in the room.
Bedtime Routine:
For children on the spectrum, bedtime routines (Figures 6 and 7) are important for them to understand the schedule of the day. This can help children fall asleep better in the evening [14].
A daily routine can lessen the anxiety of understanding what is expected at bedtime. Having a schedule can help autistic children plan to prepare to fall asleep and have wind-down time [14].

Figure 11. Bedtime Routine for Children.
It is understandable that when your child is having sleeping challenges, this can be stressful to the parent as well [7], [11]. For a bedtime routine for parents (Figure 7), the bedtime routine below is suggested:
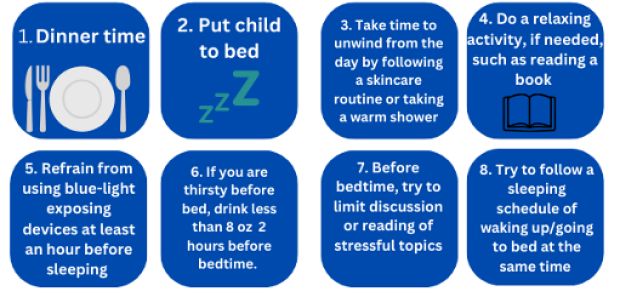
Figure 12. Bedtime Routine for Parents
B. Pharmacological Interventions
Melatonin
Melatonin is a hormone that regulates sleep-wake cycles.
• The supplement is commonly used to treat sleep disorders in individuals on the autism spectrum. The effectiveness is influenced by the type of sleep disturbance, environmental factors, and other associated medical conditions. It has been shown to improve sleep onset latency, total sleep time, and sleep efficiency [24].
• Reported but uncommon side effects include fatigue, mood swings, abdominal pain, restlessness, anxiety, constipation, diarrhea, day laziness, dizziness, drowsiness, reduced appetite, increased activity, increased excitability, headaches, migraines, trembling, nausea, vomiting, nightmares, skin pigment alterations, infections, skin rashes, and coughs [24].
• Melatonin is available as an over-the-counter medication. However, to ensure you get high-quality melatonin, you may consider having your doctor prescribe melatonin for you.
• Typical dosage is 3 to 10 mg. Typically, you will give the medication about 30 min before the intended sleep time.
• Recently, a prolonged-release formulation of melatonin has been approved for use in children on the autism spectrum. The advantages of this treatment compared to immediate-release melatonin are improvements in sleep disruption and night-time and early-morning awakenings.
Antihistamines
Antihistamines (e.g., diphenhydramine), alpha-adrenergic agonists (e.g., Clonidine, guanfacine), anti-depressants (e.g., trazodone), hypnotics (e.g., clonazepam), and atypical antipsychotics (e.g., olanzapine) have been used clinically [25]. However, these agents have not been evaluated in the autism population. In particular, a guideline has been issued by the Canadian Academy of Child and Adolescent Psychiatry against the use of atypical antipsychotics for insomnia treatment in children, adults, or the elderly as a first-line agent for the treatment of insomnia [26]
C. Complementary and Alternative Medicine
• Preliminary evidence has suggested that anti-oxidants such as L-carnosine [27] and co-enzyme Q [28] can improve sleep in children on the autism spectrum.
• The following supplements have preliminary evidence for improving sleep conditions in the non-autism population. L-5-Hydroxytryptophan (5-HTP) and gabadone have been shown to improve sleep in neurotypical individuals. [29] Natural plant-based products such as Ashwagandha had also been shown to be helpful to improve sleep [30].
• The data for iron in improving sleep in the non-autism population are mixed. Omega 3 fatty acids were shown to be ineffective in improving sleep. [29]
• For toddlers on the spectrum, sensory over-responsivity predicted late sleep difficulties, but this relationship did not hold for 4-year-olds to 10-year-olds, indicating the complexity and developmental differences in sleep-behavior relationships in autism [10].
• Obstructive sleep apnea (OSA) is common in autism. Children with OSA can present with a range of symptoms, including loud snoring, excessive daytime sleepiness, and changes in cognitive function [11].
• Children on the spectrum have a greater variability in the circadian rhythm cycle, a natural clock that helps the body fall asleep and wake up [12].