A Study of TAR-200 in Combination With Cetrelimab Versus Concurrent Chemoradiotherapy in Participants With Muscle-invasive Bladder Cancer (MIBC) of the Bladder
The purpose of study is to compare bladder intact-event free survival (BI-EFS) in participants receiving TAR-200 in combination with intravenous (IV) cetrelimab versus concurrent chemoradiotherapy.
Stanford is currently accepting patients for this trial.
Stanford Investigator(s):
Intervention(s):
- biological: Cetrelimab
- drug: TAR-200
- drug: Cisplatin
- drug: Gemcitabine
- radiation: Conventional radiation therapy
- radiation: Hypo-fractioned radiation therapy
Eligibility
Inclusion Criteria:
- Ineligible for or have elected not to undergo radical cystectomy
- All adverse events associated with any prior surgery and/or intravesical therapy must
have resolved to Common Terminology Criteria for Adverse Events (CTCAE) version 5.0
Grade less than (<) 2 prior to randomization
- Eastern Cooperative Oncology Group (ECOG) performance status Grade 0, 1, or 2
- Thyroid function tests are within the normal range per investigator assessment (or
stable on hormone supplementation). Investigators may consult an endocrinologist for
participant eligibility assessment in the case of equivocal or marginal test results
- Adequate bone marrow, liver, and renal function: Bone marrow function (without the
support of cytokines or erythropoiesis-stimulating agent in preceding two weeks):
Absolute neutrophil count (ANC) greater than or equal to (>=) 1,500/cubic millimeters
(mm^3); Platelet count >=80,000/mm^3; Hemoglobin >=9.0 grams per deciliter (g/dL);
Liver function: (Total bilirubin less than or equal to (<=) 1.5 * upper limit of
normal (ULN) or direct bilirubin <= ULN for participants with total bilirubin levels
greater than (>)1.5*ULN (except participants with Gilbert's Syndrome, who must have a
total bilirubin < 3.0 mg/dL), and Alanine aminotransferase (ALT) and aspartate
aminotransferase (AST) less than or equal to (<=) 2.5* institutional ULN); Renal
function: Creatinine clearance >=30 mL/min using the Cockcroft-Gault formula. 24-hour
creatinine clearance test will also be accepted for estimating renal function in
situations where Cockcroft-Gault formula is not a good predictor of estimating
adequate renal function
Exclusion Criteria:
- Must not have had urothelial carcinoma or histological variant at any site outside of
the urinary bladder. Ta/T1/Carcinoma in situ (CIS) of the upper urinary tract
(including renal pelvis and ureter) is allowable if treated with complete
nephroureterectomy more than 24 months prior to initiating study
- Must not have diffuse CIS based on cystoscopy and biopsy. Diffuse, or multi-focal, CIS
is defined as the presence of at least 4 distinct CIS lesions in the bladder at the
time of the Screening re-TURBT
- Participants must not have evidence of cT4b, or N1-3, or M1 disease based on local
radiology staging (chest, abdomen, and pelvis must be performed using Computed
tomography [CT] or Magnetic resonance imaging [MRI]) within 42 days prior to
randomization
- Presence of any bladder or urethral anatomic feature that, in the opinion of the
investigator, may prevent the safe placement, indwelling use, or removal of TAR 200
- Evidence of bladder perforation during diagnostic cystoscopy. Participant is eligible
if perforation has healed prior to randomization
Ages Eligible for Study
18 Years - N/A
Genders Eligible for Study
All
Now accepting new patients
Contact Information
Stanford University
School of Medicine
300 Pasteur Drive
Stanford,
CA
94305
Paige Nicole Baker
650-736-3687
I'm interested
Our research team includes physicians, residents, medical students, research assistants, and volunteers. Our research topics include medical imaging, device validation, mobile application development, and pharmaceutical trials.
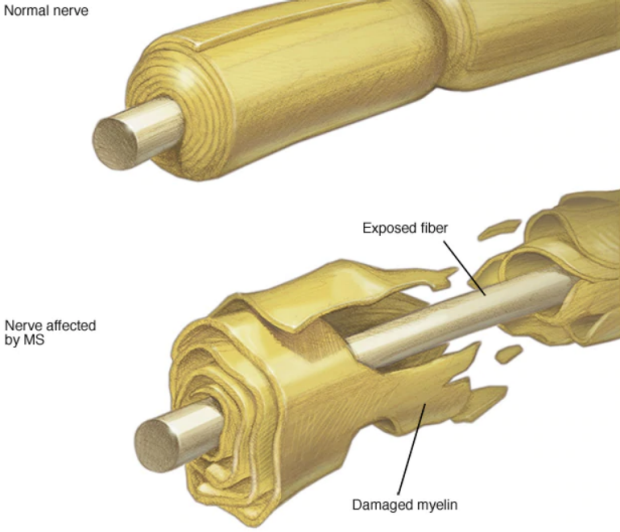
Some of the Neuro-Opthalmic concerns we investigate include Multiple Sclerosis, Optic Neuritis, IIH, and ICP.