Learning from 3D Engineered Heart Tissue
By Amanda Chase, PhD
October 16, 2020
A heart attack occurs when blood flow to the heart is blocked, resulting in oxygen loss and damage to the heart muscle due to loss of heart muscle cells (cardiomyocytes). In turn, the damaged heart muscle can disrupt the ability of the heart muscle to pump blood, resulting in heart failure. Despite the high prevalence of heart attacks and heart failure, and their high rate of morbidity and mortality, most treatment options are focused on prevention and reducing known risk factors. Cell therapy, in comparison, has the potential to offer a treatment that can treat the damage to the heart muscle and restore heart function by regenerating the damaged heart tissue.
Stem cells can be differentiated into many different specialized cells, making them an important tool for the possibilities of cell therapy. Induced pluripotent stem cells-derived cardiomyocytes (iPSC-CMs) are a potential source of cells to improve damaged heart tissue that results from heart attacks. Importantly, preclinical work suggests that they can, one day, be used in humans to treat damaged hearts. For now, this work is done in nonhuman primates and has shown that cells injected into the damaged heart tissue results in regeneration of the infected tissue.
Two ways of delivering cells to the injured heart have been developed: direct cell injection and a cell patch transplantation. Both approaches improve heart function. How they improve heart function, however, is not known. For example, how do the cells act when put into a damaged heart? How do the iPSC-CMs replace the damaged tissue? The tools to better understand those questions, and many more, were recently evaluated by a team of researchers affiliated with the Stanford Cardiovascular Institute, led by first authors Huaxiao Yang, PhD, and Ningyi Shao, PhD, and senior author Joseph Wu, MD, PhD. Their work, recently published in Cardiovascular Research, evaluated the best way to look at how heart cell therapy, or regenerative therapy, may work.
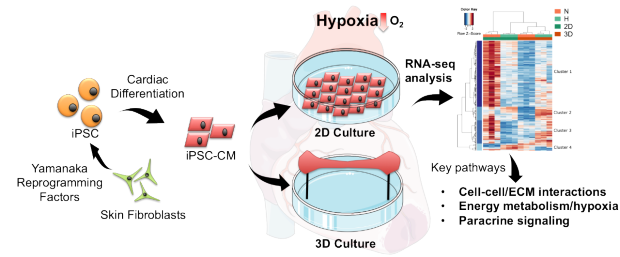
Researchers used skin cells from nonhuman primates and made them into iPSCs, which can then be made into any cell of interest. The team made them into heart cells, or cardiomyocytes (iPSC-CMs) that were then studied in a 2D monolayer or as a 3D engineered heart tissue culture. By looking at the expression of all the RNA, via RNA-seq analysis, they analyzed and compared key pathways known to be altered after a heart attack. With this analysis, they were able to show that the 3D EHT model is best for studying regenerative therapy for the heart.
Work with iPSC-CMs is historically done in a single layer on a dish, a 2D monolayer. More recently, work as moved into a 3D model with the engineered heart tissue (EHT) model, which allows for more tissue-level interactions and physiological conditions than allowed in a 2D model. The research team established and carried-out a direct comparison of the two different models to find if one was better for evaluating how cell therapy works. The different models were subjected to decreased oxygen to be similar to what is experienced during a heart attack, with normal levels of oxygen serving as a control. From the long history of research done on heart diseases, there are several identifiers known to be changed following a heart attack. The research team was able to look for those known identifiers under each of the four conditions to determine which model best represented conditions of a human heart after heart attack: the 3D EHT model. "The 3D engineered heart tissues can be easily used as a surrogate for modeling and studying ischemic cardiomyopathy, or the condition when your heart muscle is weakened from a heart attack," explains first author Dr. Huaxiao "Adam" Yang, who is now an assistant professor at the University of North Texas, Department of Biomedical Engineering. "Profiling of the iPSC-CMs under different conditions improves our understanding of the mechanism of injury that leads to decreased oxygen to the heart tissue and the chance for heart failure," says senior author Dr. Joseph Wu, "this may prove useful for advancing cell therapy delivery approaches in the future."
Other Stanford Cardiovascular Institute affiliated authors are Alexandra Holström, Xin Zhao, Tony Chour, Haodong Chen, Ilanit Itzhaki, Haodi Wu, Mohamed Ameen, Nathan Cunningham, Chengyi Tu, Ming-Tao Zhao, and Oscar Abilez.
Dr. Huxiao "Adam" Yang

Dr. Ningyi Shao

Dr. Joseph Wu