CT Perfusion Imaging in Predicting Treatment Response in Patients With Non-small Cell Lung Cancer or Lung Metastases Treated With Stereotactic Ablative Radiation Therapy
This study assesses computed tomography (CT) perfusion imaging in predicting treatment response in patients with non-small cell lung cancer or tumors that have spread from the primary site (place where it started) to the lungs (metastases) treated with stereotactic ablative radiation therapy. CT perfusion imaging is a special type of CT that uses an injected dye in order to see how blood flow through tissues, including lung tissue. CT perfusion imaging of the lungs may help doctors learn whether perfusion characteristics of lung tumors may be predictive of response to treatment and whether lung perfusion characteristics can be used to follow response to treatment.
Stanford is currently not accepting patients for this trial.
Stanford Investigator(s):
Intervention(s):
- device: CAPP-Seq
- drug: Isovue-200
- radiation: Computed Tomography Perfusion Imaging
Eligibility
Inclusion Criteria:
- Patients undergoing SABR for the treatment of a lung tumor, inclusive of non-small
cell lung cancer or lung metastases
Exclusion Criteria:
- Patients who are pregnant or are trying to become pregnant are excluded from this
study
- Patients with renal failure, defined as glomerular filtration rate (GFR) < 60 at the
time of the radiation treatment-planning (RTP) scan, will be excluded
Ages Eligible for Study
18 Years - N/A
Genders Eligible for Study
All
Not currently accepting new patients for this trial
Contact Information
Stanford University
School of Medicine
300 Pasteur Drive
Stanford,
CA
94305
Samantha Wong
650-498-8495
Not Recruiting
Our research team includes physicians, residents, medical students, research assistants, and volunteers. Our research topics include medical imaging, device validation, mobile application development, and pharmaceutical trials.
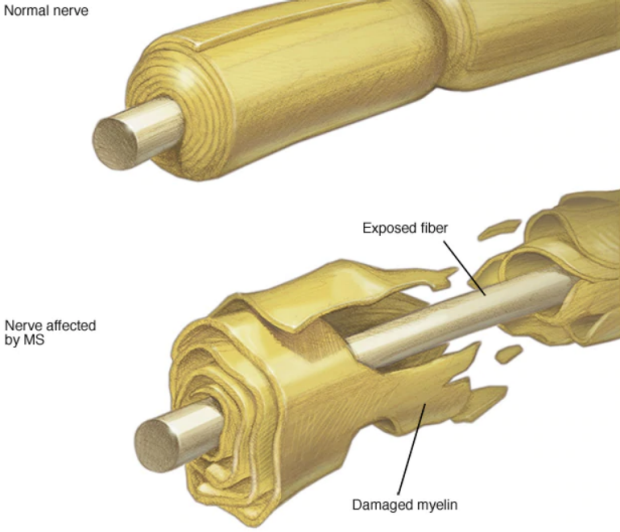
Some of the Neuro-Opthalmic concerns we investigate include Multiple Sclerosis, Optic Neuritis, IIH, and ICP.