Approach to the Exam for Aortic Regurgitation
When done properly the physical exam can not only allow us to make a diagnosis of aortic regurgitation, but also help determine its specific causes and the presence of complications like systolic and diastolic heart failure.
Introduction
Exam for Aortic Regurgitation
Aortic regurgitation is one of the most commonly encountered heart valve diseases both in the inpatient and outpatient settings. The physical exam is crucial for the diagnosis of aortic regurgitation and also for the identification of its causes and possible complications like heart failure. However, it is very important to learn the proper technique for the different sections of the exam to be 100% confident about the presence or absence of any findings. On this page we will describe the correct technique and evidence-based medicine for the different parts of the exam for aortic regurgitation, followed by the most common differential diagnoses.
Inspection and Palpation
Exam for Aortic Regurgitation
In evaluating a patient with suspected aortic regurgitation, it is important to either inspect or palpate the precordium to check the location of the Point of Maximal Impulse (PMI). Normally the PMI is at the 5th intercostal space on the left midclavicular line. However, in a patient with chronic aortic regurgitation the heart may be enlarged, and in that case the PMI will be displaced inferiorly and laterally.The physical exam of the shoulder starts by observing the patient removing his or her shirt. This is our first opportunity to notice any functional impairments of the shoulder joint.
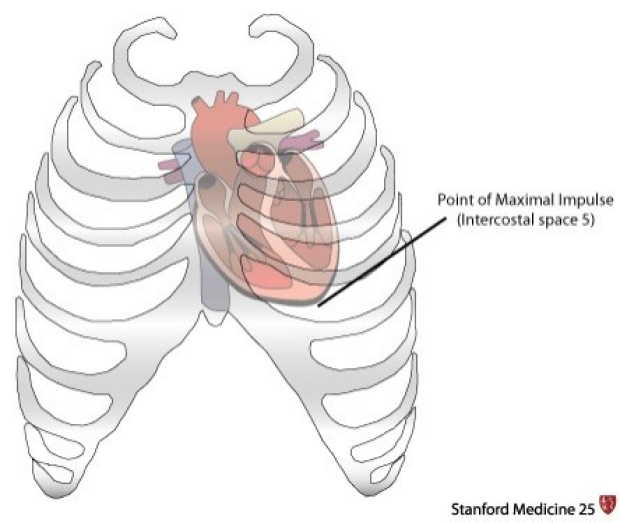
The PMI is normally at the 5th intercostal space on the left midclavicular line.
Patient positioning & palpation technique
To make it easier to appreciate the PMI it is important to have the patient assume the correct position. Ask your patient to sit upright and lean forward. Alternatively, you can ask the patient to lie down and move into the left lateral decubitus position. In both cases the heart will be closer to the chest making it easier to locate the PMI. Once the patient is in the correct position, palpate just below the nipple to appreciate the PMI. You can use either your fingertips or your full palm.

Correct patient positioning and palpation technique.
Ascending aortic aneurysm
It is also important to palpate the suprasternal notch and the 1st and 2nd right intercostal spaces. A significant pulsation here can indicate an ascending aortic aneurysm as the cause for the aortic regurgitation.
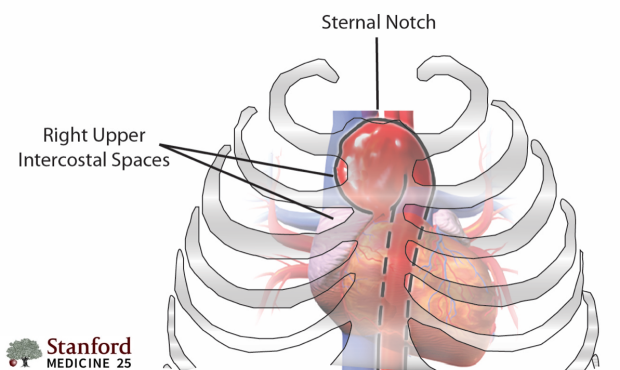
Ascending aortic aneurysm: pulsations in the right upper ICS and sternal notch.
Auscultation
Exam for Aortic Regurgitation
Auscultation is the most important part of the physical exam for aortic regurgitation. In a patient with aortic regurgitation the typical murmur is a decrescendo early-diastolic blowing murmur, best heard on the left lower sternal border, around the 3rd and 4th intercostal spaces. If this murmur is heard louder on the right sternal border, it may suggest that aortic root dilation is the cause for the aortic regurgitation. This typically occurs in the case of an ascending aortic aneurysm or aortic dissection.
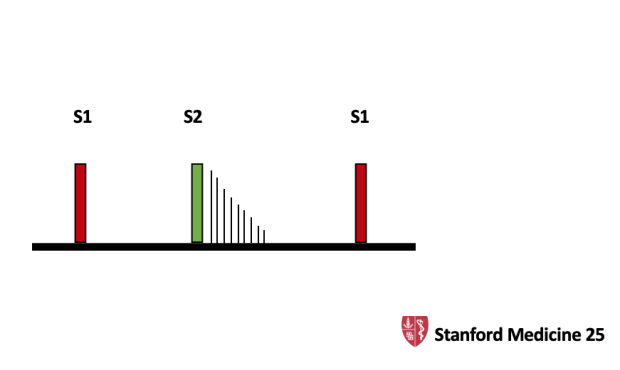
Aortic regurgitation: decrescendo early-diastolic blowing murmur.
Correct technique
As a general rule, it is useful to palpate an artery during auscultation for heart murmurs. This makes much easier to determine if a murmur is diastolic or systolic. Any artery in the upper extremity can be used for this purpose.
It's also very important to position the patient in the right way. The murmur of aortic regurgitation is indeed best heard when the patient is sitting upright, leaning forward and in full expiration. In this way the heart will be closer to chest wall and the murmur easier to appreciate. However, it is important to make sure that the patient does not exhale too forcefully, since that would cause a Valsalva maneuver that can reduce the venous return to the heart and thus the intensity of the murmur of aortic regurgitation. Also, make sure to auscultate on the right sternal border as well for the presence of aortic root dilation.
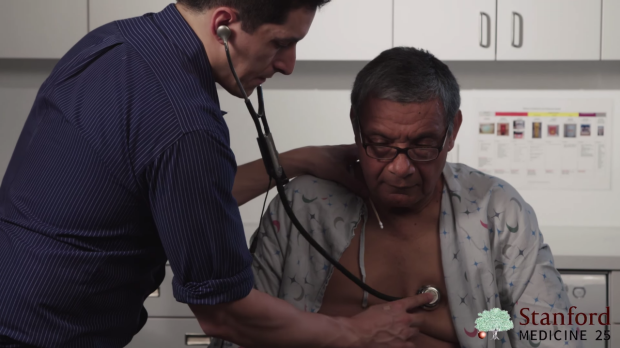
Auscultation on the left lower sternal border.
Associated murmurs: systolic flow murmur
In a patient with aortic regurgitation there is an increase in the blood flow across the aortic valve. This may generate a systolic outflow tract murmur that is best heard on the aortic area at the right upper sternal border, intercostal spaces 1st and 2nd.
This systolic murmur is usually less loud than the murmur of aortic regurgitation. For this reason, and due to the contemporary presence of the diastolic murmur, it is not always easy to appreciate.

Systolic flow murmur: right upper sternal border.
Associated murmurs: Austin-Flint murmur
The regurgitant blood flow across the aortic valve can cause a functional mitral stenosis by impacting on the anterior leaflet of the mitral valve and preventing it to fully open during diastole. This functional mitral stenosis presents as a low-pitched, mid to late diastolic murmur that is commonly referred to as Austin-Flint murmur.
Similar to the murmur of mitral stenosis, the Austin-Flint murmur can be best heard with the bell of the stethoscope at the 5th intercostal space on the left midclavicular line and with the patient in the left lateral decubitus position.
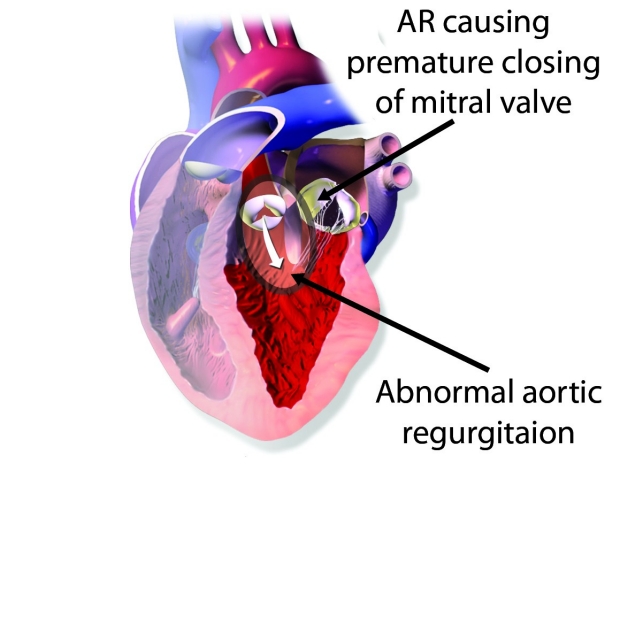
Austin-Flint murmur: pathophysiology.
Cardiac maneuvers: isometric handgrip
There are several cardiac maneuvers that can be used to better characterize heart murmurs by changing their intensity. The most useful maneuver for the exam of aortic regurgitation is the isometric handgrip.
To perform this maneuver, ask the patient to squeeze with both hands an object such as a rolled-up piece of paper. This will cause an increase in the afterload and as a consequence in the regurgitant blood flow across the aortic valve, making the aortic regurgitation murmur louder and easier to hear.

Isometric handgrip maneuver.
Other Clinical Exam Findings
Exam for Aortic Regurgitation
In a patient with aortic regurgitation the heart has to increase the stroke volume in order to keep the cardiac output constant. This causes an increase in the systolic blood pressure. At the same time there is a decrease in the diastolic blood pressure directly caused by the retrograde diastolic blood flow. This determines an increase in the pulse pressure (systolic BP – diastolic BP) which manifests with several clinical signs throughout the body that are here briefly described. It is important to note, however, that these findings are not always present since they are typical of chronic severe aortic insufficiency.
Corrigan’s pulse or sign
The Corrigan’s pulse is a bounding carotid pulse, characterized by a rapid systolic rise and a rapid diastolic collapse. To detect the Corrigan’s sign, inspect the base of the patient’s neck, right where the carotids are.

Corrigan’s sign: observe the carotids at the base of the neck.
Watson’s water hammer pulse
The water hammer pulse is a bounding pulse with rapid systolic rising and diastolic collapse that can be appreciated at either the radial, ulnar or brachial artery.
It is accentuated by slightly lifting up the patient’s arm.

Watson’s water hammer pulse: inspection.
Click here to see an example of the Watson’s water hammer pulse (ulnar artery).
The water hammer pulse can also be palpated by placing the palm of your hand on the patient’s wrist so that you can feel both the radial and the ulnar arteries. Again, it is important to lift up the patient’s arm to make it easier to detect the pulsation.

Watson’s water hammer pulse: palpation.
Quincke’s capillary pulse
Repeated flushing and blanching of the capillaries in the nail beds and lips.
De Musset’s sign
Anterior-posterior bobbing movement of the head synchronous with the arterial pulse.
Müller's sign
Back and forth pulsation of the uvula.
Becker Sign
Visible pulsations of the retinal arteries on the ophthalmoscopic exam.
Lighthouse sign
Alternate blanching and flushing of the forehead and face.
Rosenbach Sign
This sign consists in systolic pulsations of the liver that can be appreciated by palpation of the RUQ.
Gerhard Sign
This sign is described as systolic pulsations of the spleen felt on palpation of the LUQ.
Landolfi's sign
Alternating systolic miosis and diastolic mydriasis in both pupils.
Lincoln Sign
Tremor of the foot when one leg is crossed above the other, caused by excessive pulsation of the popliteal artery.
Traube’s sign (pistol-shot sound)
While auscultating over the femoral arteries it is possible to hear a pistol shot sound both during systole and during diastole. The sound can be accentuated by compressing the femoral artery with the stethoscope. The quality of this sound is very similar to the Korotkoff ones used for measurement of the blood pressure.
Duroziez sign (murmur)
This is a diastolic-systolic murmur heard when applying firm pressure with the stethoscope on the femoral arteries. The sign is positive only if both the systolic and diastolic murmurs are heard. The diastolic murmur becomes louder when more pressure is applied on the distal rim of the stethoscope.
Hill’s sign
This sign is considered positive when the difference between the systolic blood pressure measured at the foot and at the arm is greater than 20 mmHg.
Signs of Heart Failure
Exam for Aortic Regurgitation
A patient with aortic regurgitation can develop both systolic and diastolic heart failure. Once the diagnosis of aortic regurgitation is made, it is important to perform a thorough exam to identify any signs of heart failure that may be present.
Signs of systolic heart failure
Look for an S3 gallop, which develops as a consequence of heart enlargement in chronic aortic regurgitation. Other signs of systolic heart failure are peripheral cyanosis and cold and clammy extremities, both the result of poor peripheral blood flow secondary to the reduced cardiac output.
Lastly, in a patient with aortic regurgitation it is very important to calculate the pulse pressure (systolic BP – diastolic BP). Usually in presence of aortic regurgitation the pulse pressure is very high. A normal or decreased pulse pressure may indicate a reduced cardiac output and incipient systolic heart failure.
Signs of diastolic heart failure
These are signs of volume overload, both in the systemic and pulmonary circulation. In the systemic circulation the typical manifestation is peripheral edema. This usually happens in the dependent areas, that are the lower extremities in a sitting patient, and the sacrum in a bedridden patient. Another sign of systemic volume overload is jugular venous distension. Instead, volume overload in the pulmonary circulation manifests as rales on chest auscultation, which indicate pulmonary edema.
Specific Causes of Aortic Regurgitation
Exam for Aortic Regurgitation
There are many different causes of aortic regurgitation. For a complete list, look at the end of the page. Some of these conditions give specific clinical manifestations that when identified can help pinpoint the exact etiology of aortic regurgitation in your patient.
Endocarditis
Typical clinical findings include:
- Osler nodes: painful red/violaceous nodules usually found on the pads of fingers and toes;
- Janeway lesions: non painful red macules found on the palms and soles;
- Roth spots: a red hemorrhagic lesion of the retina with a characteristic white center representing fibrin-platelet plugs;
- Splinter hemorrhages: subungual hemorrhages appearing as linear non blanching brown-red lesions on the nail beds.

Osler nodes.

Janeway lesions.
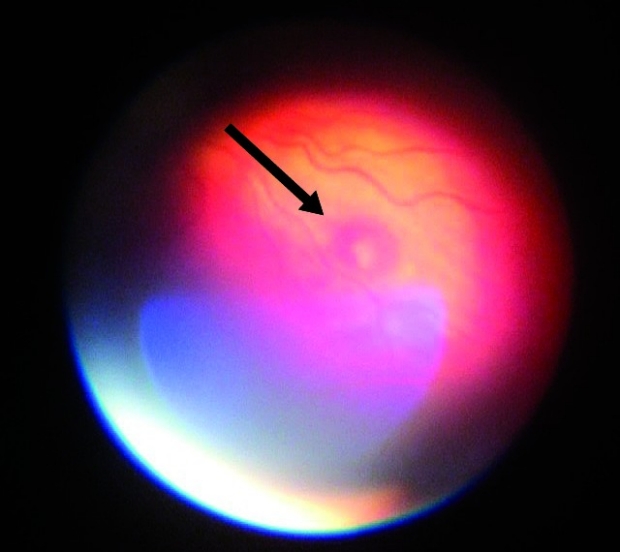
Roth spots.

Splinter hemorrhages.
Genetic Diseases: Marfan’s syndrome
Genetic diseases affecting the connective tissue, like Marfan’s syndrome can cause dilation of the aortic root and, as a consequence, aortic regurgitation.
Typical clinical findings in patients with Marfan’s syndrome include:
- Characteristic body habitus with very long limbs and fingers. These patients are usually very tall with an arm span that exceeds their height;
- Positive thumb sign: to elicit this sign ask the patient to close the fist or just to cross the thumb on the palm. If the thumb extends beyond the palm, then the sign is positive;
- Positive wrist sign: ask the patient to grip his or her hand with the other one. The sign is positive if the thumb overlaps with the fifth finger.
NB: both the thumb and wrist sign are due to the long fingers and joint hyperlaxity typical of a patient with Marfan’s syndrome.

Positive thumb sign.

Positive wrist sign.
Aortic Dissection
Patients present with severe tearing chest pain radiating to the back. Clinical signs useful to make a diagnosis include:
- Asymmetric pulses in the extremities. Look for a delayed or absent pulse on one side only;
- Difference in blood pressure between the two arms.
Infective Aortitis
Rarely seen today, infective aortitis was a common etiology of aortic regurgitation in the pre-antibiotic era. In particular, Syphilis was the most common cause.
The mechanism for aortic regurgitation in infective aortitis is the dilation of the aortic root secondary to aortic wall inflammation and damage. This results in an ascending aortic aneurysm.
Whenever an aortic aneurysm is causing aortic regurgitation there will be two characteristic signs on exam:
- Palpable pulsations on the suprasternal notch and the 1st and 2nd intercostal spaces;
- Early diastolic murmur of aortic regurgitation louder at the right sternal border rather than at the left lower sternal border.
Rheumatic Heart Disease
This is much more commonly seen as a cause of aortic regurgitation in developing countries.
Together with aortic regurgitation, such patients will almost always have rheumatic mitral valve disease presenting as mitral regurgitation or stenosis.
Chronic/Severe Hypertension
Patients with long standing severe hypertension may develop aortic valve disease usually manifesting as aortic regurgitation (secondary to dilation of the aortic root).
Since chronic severe hypertension damages blood vessels all over the body, in these patients it is possible to observe characteristic vascular lesions and ischemic changes on the retinal exam, like flame hemorrhages and cotton wool spots.
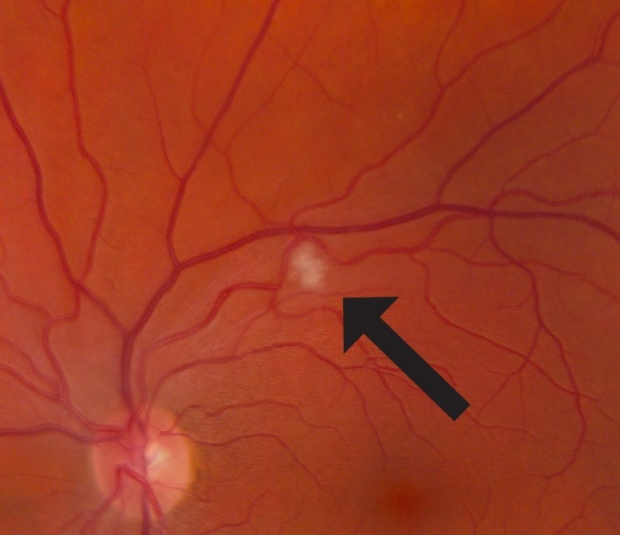
Fundoscopy: Cotton Wool Spots.

Fundoscopy: Flame hemorrhage.
Evidenced-Based Medicine*
Exam for Aortic Regurgitation
*Credit goes to “Evidenced-based physical diagnosis - 4th ed”, Steven McGee, MD.
Here we describe the most significant evidence supporting the clinical utility of different signs and techniques in the exam for aortic regurgitation.
Inspection & palpation
The absence of an enlarged or sustained PMI reduces the chances that aortic regurgitation is present by almost 45% (negative Likelihood Ratio of 0.1).
Auscultation
The characteristic murmur of aortic regurgitation, early diastolic louder at the left lower sternal border, has a positive Likelihood Ratio of 9.9 for the diagnosis of mild or more severe aortic regurgitation. This means that hearing this murmur on physical exam increases the probability that aortic regurgitation is present by roughly 45%.
On the other hand, this finding has a negative Likelihood Ratio of 0.1 for moderate to severe aortic regurgitation. The clinical implication is that not detecting the characteristic early diastolic murmur of aortic regurgitation will decrease the probability that an aortic leak is actually present by almost 45%.
When the early diastolic murmur of aortic regurgitation is heard louder on the right sternal border there is a 30-45% increase in the probability that a dilated aortic root is the cause for the aortic regurgitation (positive Likelihood Ratio of 8.2).
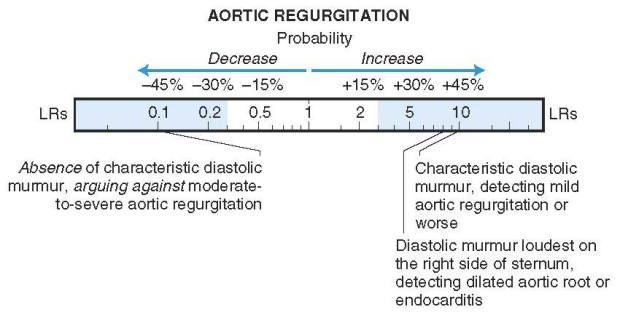
Auscultation for aortic regurgitation: evidence-based medicine.
Blood pressure
In a patient presenting with the characteristic murmur of aortic regurgitation, the following blood pressure changes have a high diagnostic utility:
- Diastolic blood pressure < 50 mmHg (positive Likelihood Ratio 19.3 à more than 50 % increase in the chances that aortic regurgitation is present)
- Pulse pressure > 80 mmHg (positive Likelihood Ratio 10.9 à more than 50 % increase in the probability that the patient has aortic regurgitation).
Hill sign
The Hill sign is positive if there is more than 20 mmHg difference in the systolic blood pressure between the arm and the foot. If the cutoff for positivity is moved up to more than 60 mmHg difference, the sign has a positive Likelihood Ratio of 17.3 for the presence of aortic regurgitation (increase in the probability that aortic regurgitation is present by more than 50%).
Differential Diagnoses
Exam for Aortic Regurgitation
Aortic regurgitation can be caused either by primary damage to the valve leaflets, or by dilation of the aortic root that prevents the valve from closing completely during diastole. In some cases, both mechanisms are present at the same time.
Accordingly, one way to classify the etiologies of aortic regurgitation is the following:
- Primary valve damage
o Infectious endocarditis
o Rheumatic valve disease
o Calcific aortic valve disease (even though most commonly manifests as aortic stenosis)
o Myxomatous degeneration
- Primary aortic root dilation
o Chronic severe hypertension
o Marfan’s syndrome
o Ehlers-Danlos syndrome
o Giant cell arteritis
o Takayasu arteritis
o Infectious aortitis
- Contemporary valve damage and aortic root dilation
o Aortic dissection
o Ankylosing spondylitis
o Bicuspid aortic valve
Key Learning Points
Learn the shoulder exam aspects that include:
- inspection
- palpation
- provocative tests
- neuro exam
- awareness of more concerning causes
Related to Aortic Regurgitation Exam
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam