Approach to the Exam for Diastolic Murmurs
Diastolic murmurs are commonly encountered findings on the auscultation of the heart, both in the outpatient and inpatient setting. The physical exam, when performed correctly, can by itself help determine the underlying cause of a diastolic murmur.
Introduction
Exam for Diastolic Murmurs
Diastolic murmurs are always a pathological finding on the auscultation of the heart, indicating the presence of a valvular abnormality. The physical exam can, by itself, reveal the cause of a diastolic murmur. However, it is very important to perform the physical exam with the right technique in order to maximize our chances to identify a diastolic murmur and determine its cause. On this page we will review the four most common types of diastolic murmurs with a particular focus on their causes and the best approach to the physical exam. We will also briefly review some of the most common causes for a continuous murmur.
Aortic Regurgitation
Exam for Diastolic Murmurs
There are multiple causes for aortic regurgitation. One approach to classify them could be to differentiate between acute and chronic processes. The most important causes of acute aortic regurgitation are infective endocarditis and aortic dissection. Instead, the most common causes of chronic aortic regurgitation are aortic root dilation secondary to chronic hypertension and calcific degenerative aortic valve disease.
Auscultation technique
The murmur of aortic regurgitation is loudest at the left lower sternal border, around the 3rd and 4th intercostal spaces. Also, any maneuver that brings the heart closer to the chest wall will increase the intensity of this murmur. To do this, the best approach is to ask the patient to sit upright on the examination table, lean forward and hold the breath in full expiration. If the diastolic murmur is caused by aortic regurgitation it should increase in intensity with these maneuvers.

Auscultate at the LLSB with the patient sitting upright.
Bounding arterial pulse
In a patient with aortic regurgitation there is an increase in the differential blood pressure (systolic blood pressure – diastolic blood pressure). This is caused by both an increase in the SBP, secondary to a greater stroke volume, and also by a reduction of the DBP as a consequence of the regurgitant blood flow during diastole. The increased differential pressure manifests as a bounding arterial pulse that can be appreciated basically at any artery around the body. For this reason, there are many different peripheral signs of aortic regurgitation, based on the specific artery considered. The most famous ones are the Corrigan’s pulse, visible at the carotids, and the Water-Hammer pulse, that can be observed at the wrists.


Pulmonary Regurgitation
Exam for Diastolic Murmurs
Pulmonary regurgitation is a relatively rare cause of a diastolic murmur, and it is usually due to either infectious endocarditis or pulmonary hypertension. In the first case, there is direct damage to the valve leaflets caused by an infectious process. In the second case, instead, there is a dilation of the pulmonary artery root that causes the valve to become incompetent.
Differentiation from aortic regurgitation
The diastolic murmur of pulmonary regurgitation is very similar to the one of aortic regurgitation. It is a decrescendo diastolic murmur with a blowing character. However, contrary to the one of aortic regurgitation, this murmur is loudest at the left upper sternal border, around the 2nd and 3rd intercostal spaces. Because of their similarity, it can be very difficult to differentiate between these two murmurs relying on auscultation alone. The key differential element is the presence of a peripheral arterial bounding pulse, that only patients with aortic regurgitation will demonstrate.
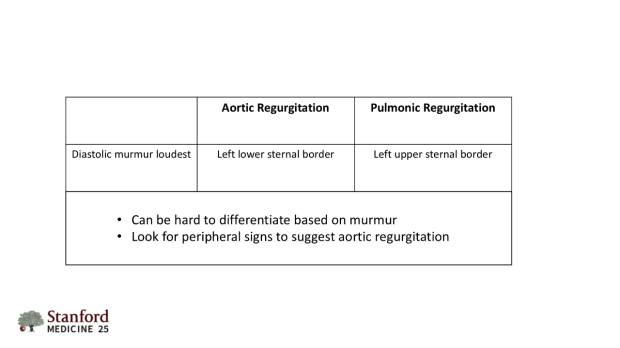
Differences between aortic and pulmonic regurgitation.
Mitral Stenosis
Exam for Diastolic Murmurs
One of the most common causes of a diastolic murmur is mitral stenosis. It is the most common manifestation of rheumatic heart disease, which is also the main etiology of mitral stenosis. Other less frequent causes of mitral stenosis are atrial myxoma, calcific annular degeneration of the mitral valve and congenital causes, which are seen mostly in the pediatric population.
Auscultation technique
The murmur of mitral stenosis is heard loudest at the 5th intercostal space on the midclavicular line, approximately around the area of the left nipple. Also, it is heard best using the bell of the stethoscope and with the patient in the left lateral decubitus position. This murmur presents as a low-pitched diastolic rumble usually preceded by an opening snap, which is an extra sound heard soon after S2.

Auscultation for mitral stenosis: correct patient positioning.
Tricuspid Stenosis
Exam for Diastolic Murmurs
Tricuspid stenosis is the rarest of all causes for a diastolic murmur. Usually, it is found in patients with rheumatic heart disease. In this case, the patients will also have either mitral valve disease, aortic valve disease or both, making it hard to appreciate the murmur of tricuspid stenosis. The most important cause of isolated tricuspid stenosis is instead carcinoid syndrome.
Auscultation technique
The murmur of tricuspid stenosis is heard best at the left lower sternal border using the bell of the stethoscope, similarly to the murmur of mitral stenosis. Also, we can increase the intensity of the tricuspid stenosis murmur by asking the patient to take a deep breath, thus increasing the blood flow to the right side of the heart and across the stenotic valve. Lastly, in isolated tricuspid stenosis there will be a fixed split S1, secondary to the delayed closure of the stenotic tricuspid valve.

Auscultation for tricuspid stenosis.
Continuous Murmurs
Exam for Diastolic Murmurs
It is important to differentiate diastolic and systolic murmurs from continuous murmurs, that are heard both in systole and in diastole. We will briefly describe two of the most common causes of a continuous murmur, that are the patent ductus arteriosus and pericarditis.
Patent ductus arteriosus
The ductus arteriosus connects the pulmonary artery and the aorta during fetal life, allowing the passage of oxygenated blood from the right to the left side of the heart. Normally it closes right after birth when the pressure in the pulmonary circulation increases. However, if the ductus arteriosus stays open it will be possible to appreciate a continuous murmur that is loudest at the left infraclavicular area. This murmur is continuous since the blood pressure in the aorta is higher than the pressure in the pulmonary artery both during systole and during diastole. This allows for a continuous blood flow across the defect.
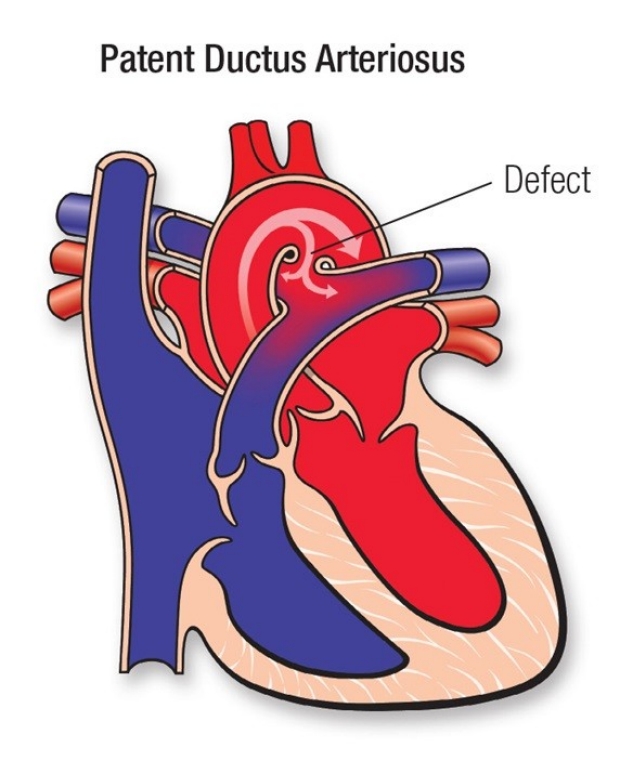
Patent Ductus Arteriosus (credit to the American Heart Association).
Pericarditis
In patients with pericarditis, it is often possible to auscultate a pericardial friction rub, generated by the attrition between the inflamed layers of the pericardium during the cardiac cycle. Since the pericardial layers are always in contact with one another, the friction rub will be heard both in systole and in diastole. Even though not technically considered a murmur, it can be easily mistaken for one. However, its grainy quality helps to distinguish the pericardial friction rub from a murmur.
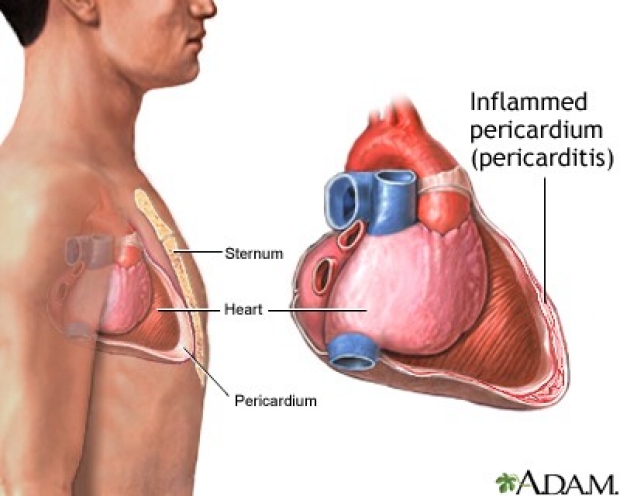
Pericarditis (credit to medlineplus.gov)
Key Learning Points
Learn the diastolic murmurs exam aspects that include:
- aortic regurgitation
- pulmonary regurgitation
- mitral stenosis
Related to Diastolic Murmurs Exam
The Stanford Medicine 25
- Aortic Regurgitation Exam
- Ankle Brachial Index
- Ankle and Foot Exam
- Ascites & Venous Patterns
- Bedside Ultrasound
- Breast Exam
- Cardiac Second Sounds
- Carpal Tunnel Exam
- Cerebellar Exam
- Deep Tendon Reflexes
- Dermatology Exam: Acne vs. Rosacea
- Dermatology Exam: Learning the Language
- Dermatology Exam: Nevi (Mole) Exam
- Fundoscopic Exam (Ophthalmoscopy)
- Gait Abnormalities
- Hand Exam
- Hip Region Exam
- Internal Capsule Stroke
- Involuntary Movements and Tremor Diagnosis: Types, Causes, and Examples
- Knee Exam
- Liver Exam
- Low Back Exam
- Lymph Node Exam
- Neck Vein Exam
- Pelvic Exam
- Precordial Movements in the Cardiac Exam
- Pulmonary Exam: Percussion & Inspection
- Pupillary Responses
- Pulsus Paradoxus and Blood Pressure Measurement Techniques
- Rectal Exam
- Spleen Exam
- Tarsal Tunnel Exam
- Thyroid Exam
- Tongue Exam
- Liver Disease, Head to Foot
- Visit the 25
- Shoulder Exam Tutorial
- Parkinson's Disease Exam
- Diastolic Murmurs Exam
- Dermatology Exam: Nevi (Mole) Exam