A Diagnosis of Nelson's Syndrome and Why You Won't See it Anymore
December 5, 2019
Author: Baffour Kyerematen, Medical Student

The Beginning
At age 15, Gillian noticed changes in her body that did not feel typical of a young adolescent woman. While a relatively thin-framed and jovial adolescent, she slowly became easily fatigued during day-to-day behaviors and was marked by an unusual weight gain, primarily in the face, abdomen, and back of her neck. In addition to stretch marks on her hips and thighs, an atypical growth of facial hair, and cessation of her menstrual cycle, her symptoms appeared out of the ordinary for a normal course of puberty. After only six weeks, a noticeable shift in her personality to a more reclusive and introverted demeanor prompted her parents to seek more robust medical attention. She was soon diagnosed with Cushing Disease. After a year of monitoring her cortisol levels with little to no reduction in signs and symptoms, she underwent a double adrenalectomy at age 16, which was the customary procedure for this diagnosis in 1973. Within 6 months of her procedure, Gillian felt like her normal self and made the presumption that the procedure treated her condition. However, a short two years later, she noticed that her skin began to darken considerably.
What is the cause of this sign?
HPA Axis and Cushing Disease
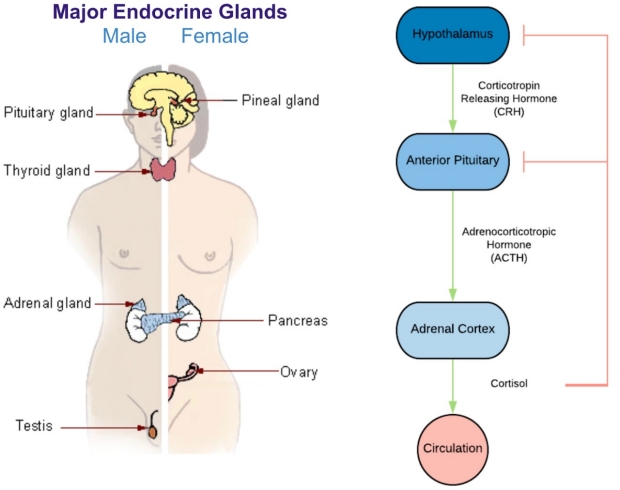
In a normally functioning endocrine system, cortisol is released by the adrenal glands, which are endocrine organs located just superior to the kidneys. The adrenal glands are a part of the overall Hypothalamic-Pituitary-Adrenal Axis, which regulates various hormones that result in cortisol production (see diagram below). Cortisol is produced by the cortex of the adrenal gland by stimulation from the anterior pituitary and hypothalamus in the brain. Cortisol is also responsible for inhibiting the anterior pituitary and hypothalamus in a method to regulate its own production.
After reaching a certain threshold, the circulating cortisol should cause a reduction in anterior pituitary and hypothalamic production of stimulating hormones, thus reducing cortisol production to keep a balance. However, if the amount of circulating cortisol continues to increase without inhibition, there is a likely disruption to the system.
Cushing Syndrome is a condition of signs and symptoms that result from exposure to elevated levels of circulating cortisol. Typically, the high cortisol level that results in Cushing Syndrome is caused by either one of two different pathways: (1) medication-induced via “cortisol-like” medications, such as prednisone or (2) a tumor that either produces cortisol or promotes increased cortisol production.
In Gillian’s case, she was not taking any cortisol-like medication, therefore pathway 1 would not be highly indicated. What remains is the possibility of either a cortisol secreting tumor or a tumor that results in increased cortisol production. By testing her adrenocorticotropic hormone (ACTH) levels, a hormone released by the anterior pituitary, we can identify if her levels are elevated, which would suggest a pituitary adenoma that is releasing ACTH into her circulation. ACTH would then stimulate the cortex of her adrenal glands to produce cortisol, and the subsequent large amounts of cortisol produced would not effectively inhibit the ACTH released from the pituitary adenoma. This type of secondary hypercortisolism that results from excessive production of ACTH by a pituitary adenoma is specifically known as Cushing Disease.
The initial treatment back in 1973 was to first remove adrenal glands to cause immediate reduction of cortisol levels. It was believed that by doing this first, you control the signs and symptoms of hypercortisolism. However, we now know this approach is not the preferred first-line treatment in those with pituitary tumors. It is true that removing the cortisol-producing adrenal glands will reduce the symptoms of hypercortisolism. However, the underlying pathology stems from the overproduction of ACTH from the anterior pituitary, not a sick adrenal gland. Therefore, removing the adrenal glands does not effectively reduce the elevated circulating ACTH levels. Instead the opposite is often observed, and the risk of increased tumor size is also indicated. One of the various complications of elevated ACTH levels is Nelson’s Syndrome, often marked by hyperpigmentation in the skin, most evidently seen in the joints.
Further Complications
Increased levels of ACTH can lead to an increase in melanocyte production, which is the cell type in the skin responsible for producing melanin, the pigment observed in skin color. Particularly in patients with lighter skin color, this characteristic darkening observed in Nelson Syndrome is especially noticeable. Primary to her darkening skin, the increasing size of the pituitary adenoma was the chief concern. At age 18, Gilian underwent pituitary radiation to reduce the impending tumor. The procedure was only minimally effective, and her skin remained dark along with her other life-interrupting symptoms. In 1978, at the age of 21 she underwent transsphenoidal partial resection of the pituitary tumor. Her ACTH levels fell, along with some of her symptoms. Although, five years later, ACTH was once again elevated. In 1983 (now 26 years of age), she underwent another pituitary resection via craniotomy to remove the superior aspect of the once again enlarged tumor. She again experienced a reduction in symptoms due to the reduction in ACTH levels. Unfortunately the very next year, her symptoms returned for a third time along with the increase in ACTH.
The Breaking Point and Resolution
Faced with the disheartening information that there was nothing more her physicians could do, Gillian took matters into her own hands and began researching physicians in the United States who could help her.

Gillian age 15, diagnosis of Cushing’s (left). Use of photo granted by patient. Gillian age 16, 6 months post adrenalectomy (right)
After a few unsuccessful attempts at US medical centers, she connected with the late Dr. Charles Wilson of the University of California San Francisco. Dr. Wilson was an integral factor in the findings against bilateral adrenalectomies as the first-line treatment in the diagnosis of Cushing’s disease. With Dr. Wilson, Gillian underwent a transfrontal surgery through the mouth and underwent 6 weeks of additional radiation to stabilize her pituitary adenoma. After a small bout of radiation sickness, her tumor size was stabilized for about 20 years.
However, her skin remained dark and did not re-lighten unlike some of her previous treatments.

Gillian, age 51 (2010). Use of photo granted by patient.
In 2010, her endocrinologist back in London noticed that her skin was darkening again. The pituitary adenoma was now resting behind her right eye, and she experienced some intracranial bleeding and eventual apoplexy. Her right pupil remained enlarged as the tumor created pressure on her oculomotor nerve. In lieu of her symptoms, she visited Dr. Laurence Katznelson at Stanford Medical Center due to his practice of prescribing the at-the-time experimental drug, pasireotide, for Cushing disease treatment. Throughout these treatments, she lost most of the hyperpigmentation that had been present for decades within six months. Her ACTH levels dropped considerably over six months with monthly Pasireotide injections.
The new normal
After multiple decades of recurring symptoms and procedures, Gillian was able to reach a point where her tumor was stabilized and her symptoms markedly reduced. She lost the dark pigmentation from her skin, knuckles, elbows, and other joints. Although her tumor was too near her optic nerve for full treatment via cyberknife radiation, the pasireotide stabilized her tumor and Gillian’s quality of life greatly improved. She now remains engaged with Dr. Katznelson’s work at Stanford Medical Center and his involvement with the pasireotide experimental board. Today, she remains thankful that she was able to undergo these treatments to reach a place of stability. Gillian contributes her time as a member of the UK Pituitary Foundation to help educate physicians and patients alike on Cushing Disease and associated symptoms and treatments.
Thank you to Gillian Lawrence for allowing us the privilege to share her story, and Errol Ozdalga, MD and Laurence Katznelson, MD and for their contributions to this article.