The Spine Sign
We are pleased and excited to announce the formation of the Society of Bedside Medicine, which began through connections built at the Stanford 25 Bedside Medicine Symposium. An international group of physician educators came together to launch the society with a focus on reinvigorating bedside medicine and education.
We hope that many users of the Stanford 25 will be excited to join the Society of Bedside Medicine and enjoy the educational tools and benefits that membership provides. Please see our website to learn more - https://bedsidemedicine.org/
One user benefit is access to our bedside teaching guides called the five minute bedside moment. They are designed to be used by a bedside educator whenever one has a few minutes at the bedside. Here is an example you might use for point-of-care ultrasound teaching:
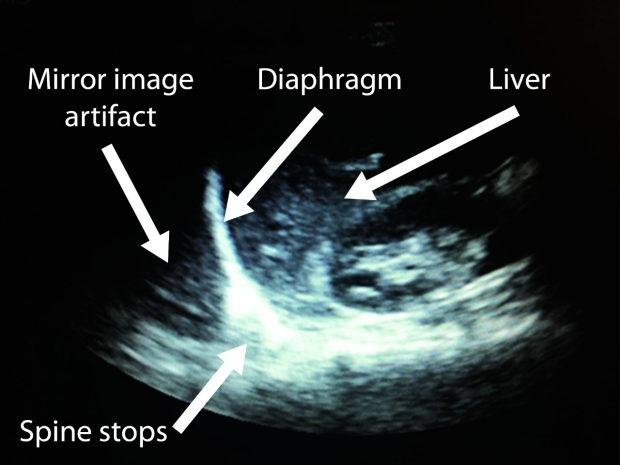
No spine sign present
Point-of-care ultrasound (POCUS) has a sensitivity and specificity for pleural effusions of 93% and out performs chest x-ray in detecting and characterizing pleural effusions. Using POCUS physicians are able to detect as little as 5ml of pleural fluid. Nevertheless deciding if a patient has pleural fluid is not always easy. Aerated lung and most pleural effusions show up dark grey on ultrasound which is why the spine sign is so helpful. In patients without a pleural effusion the spine is obscured by air in the lung, so the spine is cut off at the diaphragm. In patients with a pleural effusion the spine is visible beyond the diaphragm.
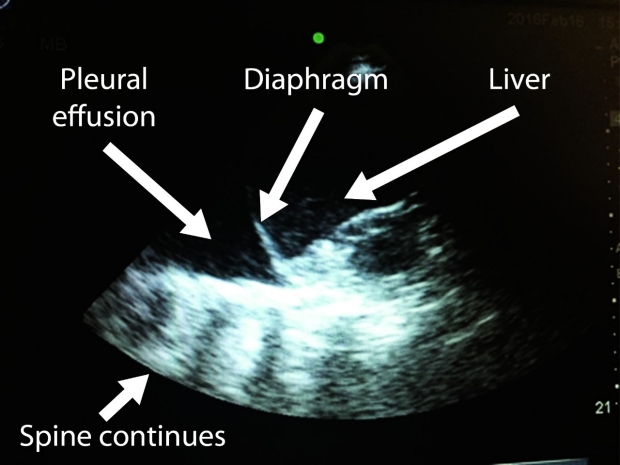
Spine sign present
Technique: The patient should be lying on their back with the head of the bed slightly elevated. Place the cardiac probe (can also use a micro convex or even curvilinear probe) along the posterior axillary line with the probe indicator oriented superiorly at the level of the 7th or 8th intercostal space. Slide the probe superiorly or inferiorly until the diaphragm is close to the center of the screen. Fan the beam anterior and posterior until you locate the thoracic spine
Clinical Utility: Evaluation for a pleural effusion should be part of the approach to any patient with hypoxia or shortness of breath. Additionally when performing a comprehensive volume status assessment it is important to observe for pleural effusions.
Reference: Soni, Nilam J., MD; Arntfield, Robert, MD; Kory, Pierre, MPA, MD. Point of Care Ultrasound. Elsiver 2015 Chapter 10