Disparities in Quality of Care
Disparity Dashboard
Supported by funding from the National Institute of Health, we are developing a disparity dashboard that will enable comprehensive assessment of racial/ethnic differences in the quality of NICU care. The disparity dashboard will allow providers to see how well their unit is performing on a variety of key quality measures, as measured by the Baby-MONITOR, with options to compare outcomes within each measure by race/ethnicity. The dashboard will provide feedback of disparity scores to NICUs and will serve as the starting point for promoting disparity solutions.
Our recent publication in Pediatrics showed that there are racial and ethnic disparities in the quality of care received by infants in the NICU. The graph below shows overall Baby-MONITOR scores by race/ethnicity for 40 California hospitals. African-American and Hispanic infants received worse care overall, although the differences were not uniform. Certain hospitals actually provided better care to these groups, but the best performing units tended to deliver better care to white infants. However, hospital care may not necessarily be the biggest contributor to these disparities; future work will examine the social and environmental factors that could be contributing to poorer outcomes among minority populations.

Effects of Social and Built Environment
Racial/ethnic disparities in the quality of care provided in neonatal intensive care units to very low birth weight infants result directly in avoidable death and morbidity. National health policy recommendations for reducing disparities call for investigating the multi-level factors that influence NICU quality. We are developing comprehensive models of quality of NICU care that explicitly include social and neighborhood level factors in additional to maternal and infant clinical and hospital factors. Appraisal of multilevel factors associated with NICU quality will promote fairer comparisons across NICUs by making the influence of social and built environment explicit and help assess key areas of quality including processes and outcomes of care that modulate long-term neurodevelopmental outcomes.
Related Publications:
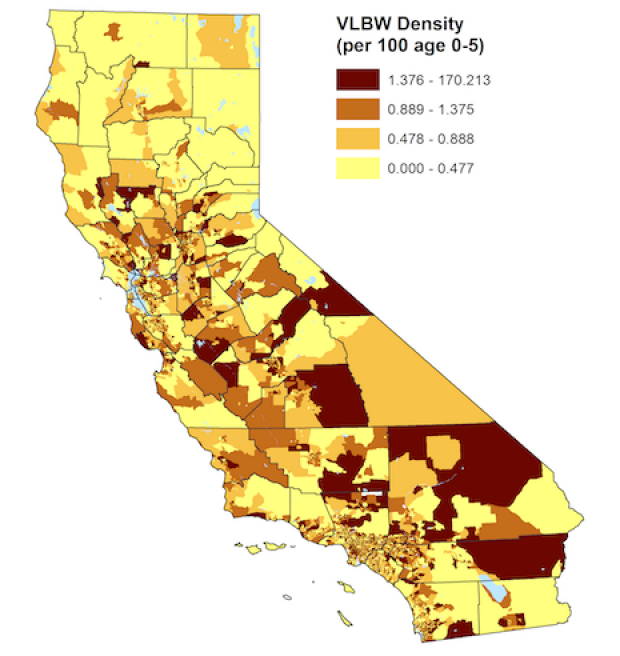
PAS 2017 Poster on Social and Built Environment Factors and VLBW rates
Qualitative Analysis of Disparity
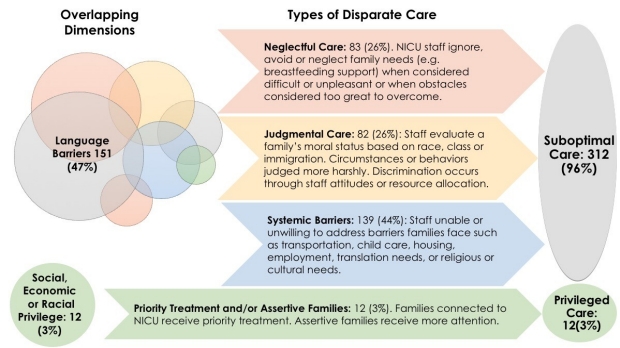
Our previous research has shown that racial and ethnic disparities exist in the clinical care of neonates, but little is known about how families experience these differences. The Profit Lab team collected and analyzed 324 individual anecdotes of disparities in care, solicited from more than 1000 clinician and family advocate attendees of the Vermont Oxford Network (VON) Quality Congress in 2016. The vast majority of stories of perceived disparate care resulted in perceived worse care. Based on Dr. Krista Sigurdson’s analysis, stories were grouped into three broad themes: neglectful care, judgmental care, and systemic barriers to care.
- Neglectful care: The NICU staff provided less time or attention to families who were perceived as having unrealistically high needs, cultural differences, and/or who didn’t speak English, (85 stories/26%).
- Judgmental care: Families were evaluated on their moral status by the NICU staff. Families’ behaviors or circumstances were perceived to be judged differently based on race/ethnicity, socioeconomic status, or history of drug use, (85 stories/26%).
- Systemic barriers to care: Systemic, organizational, or cultural barriers to care prevented families from being able to be present in the NICU or behave in a way that was congruous with the institutional culture of the NICU. This category represents the largest number of stories, (142 stories/44%).
Based on the results of this study, CPQCC is exploring methods for measuring how well a NICU is able to partner with families. Family-centered care is the standard of care for NICUs and pediatrics in general. It aims to support families and respect each individual family’s needs and cultural preferences. A growing body of research is exploring the ways family-centered care is better for families and babies in the NICU, and while guidelines for providing family-centered care aren’t new, implementation varies widely. In the coming weeks, CPQCC will be rolling out a series of action ideas for units looking to improve their adherence to family-centered care practices for diverse families.
Three sample action ideas to improve family-centered care (from CPQCC Tip Sheet):
- Signal importance of family-centered-care. Provide multi-lingual signage welcoming all families as partners in care. For example: “NICU families, we welcome you as partners in your child’s care at ALL times.”
- Offer opportunities for families to interact with their babies and care team in ways that works for family (e.g. by phone, in person or through remote participation tools such as webcams or iPads).
- Offer language assistance (translation and multi-lingual materials) to families with limited English proficiency, especially during critical phases of care (e.g. consider a translator on rounds, seek language concordance between providers and families).
Related Publications:
Disparities in NICU Quality of Care: A qualitative study of family and clinician accounts