A Compilation of our Accomplishments and Recognitions
Lab Highlights
Sep September 01 Wed 2021
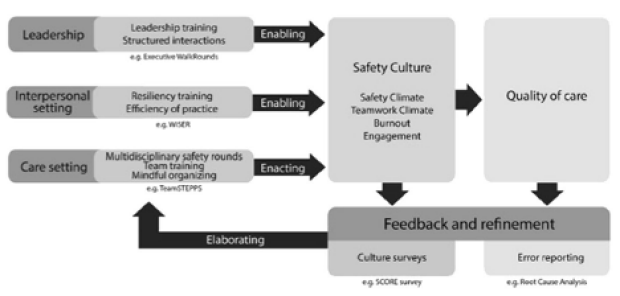
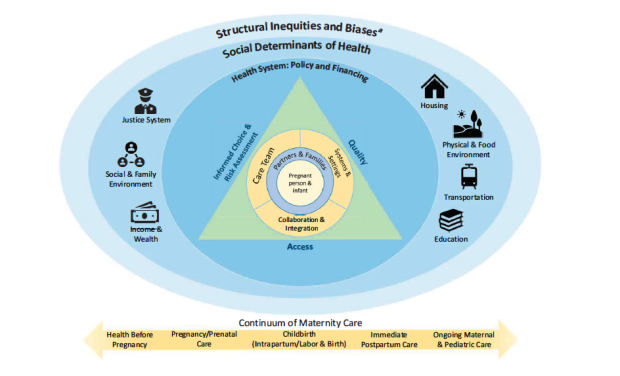
Dr. Profit, Dr. Dhurjati, and Dr. Elliott Main (from CMQCC) worked together on a commentary related to institutional racism in perinatal health in Pediatrics.
The research team comments here on a Glazer et al issue in the same Pediatrics issue that reported a higher risk of complications in Black and Hispanic term infants in New York City. The Glazer study is the latest in a body of literature describing that infants born to mothers from vulnerable populations are more likely to be sorted into lower-performing hospitals. The authors suggest a few policy solutions that could address this long-standing problem. One potential solution is the implementation of quality improvement collaboratives that could improve quality of care and performance and better meet the needs of vulnerable populations. The second potential solution would be to steer patients from vulnerable populations to better performing hospitals, although concerns about transportation and Medicaid reimbursement below cost for the receiving hospitals could make this solution difficult in practice. A third solution described a model of hospital co-ownership that results in a more efficient regionalized care system. The authors argue ultimately that the Glazer study needs to be replicated in other geographic regions of the US to shed light on geographic variation in quality of care for vulnerable mothers and infants.
KEY TAKEAWAY: Segregated and unequal care contributes to differences in quality of care for mothers and infants from vulnerable communities, and the delivery hospital may play a large role in this variation.
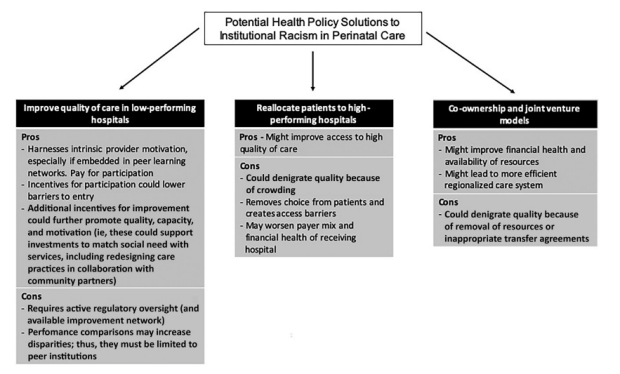
Figure 1. A solutions-focused policy framework to address institutional racism and improve care delivery at hospitals that predominantly serve vulnerable populations.
Aug August 09 Mon 2021
Dr. Jochen Profit and co-authors from CPQCC and the Duke Center for Healthcare Safety and Quality reported strong efficacy for reducing healthcare worker (HCW) burnout in participants of the WISER intervention study in Journal of Perinatology.
Health care workers (HCWs) are at high-risk for burnout due to the emotional challenges of clinical care and changes in technology and guidelines. Burnout has been linked to increased HCW attrition, staffing shortages, higher rates of infections, and self-reported errors. With only a few effective interventions to address burnout, the authors developed and refined a program known as the web-based implementation for the science of enhancing resilience (WISER). The stepwise program is delivered via mobile platform and consists of evidence-based interventions shown to improve well-being and reduce depression symptoms. The components of WISER are designed to encourage participants to gradually savor positive emotions and eventually to actively elicit them with time and practice. The lead authors conducted a clustered randomized controlled trial (RCT) to test the effectiveness of the intervention. WISER was administered to HCWs at eight NICUs randomized into two cohorts of four NICUs each. Results of the WISER intervention demonstrate reduced burnout in participating NICU HCWs when compared to controls at the 1-month and 6-month intervals.
KEY TAKEAWAY: The WISER program was shown to be effective in reducing the emotional exhaustion component of burnout and was associate with significant improvement in other aspects of well-being. Participation in a low-burden, no-cost well-being intervention such as WISER presents a promising avenue for health care institutions to address burnout in their HCWs.
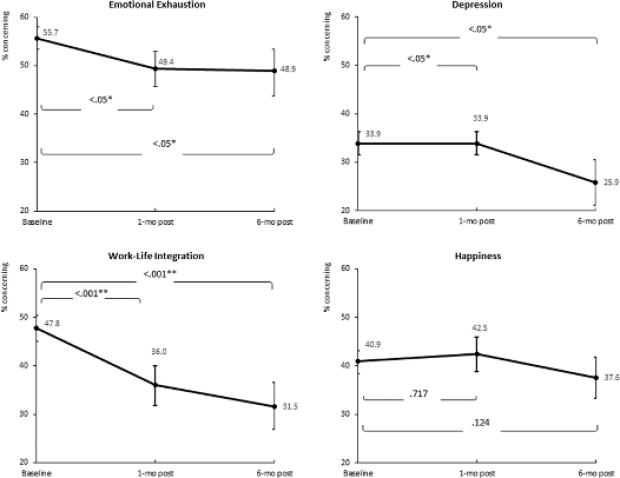
Figure 2. Statistical comparisons between combined cohort baseline to 1-month post and 6-month post provided in brackets.
Aug August 01 Sun 2021
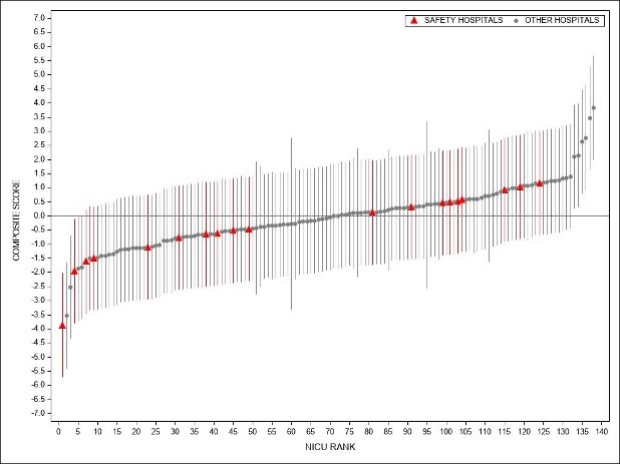
Dr. Profit and colleagues from the Vermont Oxford Network (VON) worked on a study aiming to use the Baby-MONITOR index measure to evaluate NICU care quality by race and ethnicity across and within NICUs in the US in Journal of Pediatrics.
The research team used the Baby-MONITOR index score and its component measures to study differences in quality of care by race and ethnicity in the US within and across NICUs. The population studied included 169,400 very low birthweight and very preterm infants from 737 VON hospitals born between 2015 and 2019. Baby-MONITOR scores were derived from collected process and outcome measures that were standardized relative to other units in the dataset and weighted. Researchers calculated compatibility intervals for summary scores and performed a sensitivity analysis to assess the effects of selection bias in the data. Results of the study showed African American, Hispanic and Asian American infants had positive average summary scores when compared with white infants, whereas American Indian infants had lower summary scores. Differences between racial/ethnic group on summary scores varied by domain, while differences between NICUs were similar to those observed within NICUs. All 4 minority groups scored higher on average outcome measures as compared to white infants. The research team conclude that summary scores provide a look into average measures across racial/ethnic groups, but likely mask important variance in quality of care provided to infants inherent in a composite index.
KEY TAKEAWAY: The research team identified variation in quality of care provided across and within NICUs for different racial/ethnic groups, but the findings suggest further research on the relationship between race/ethnicity and process and outcome measures.
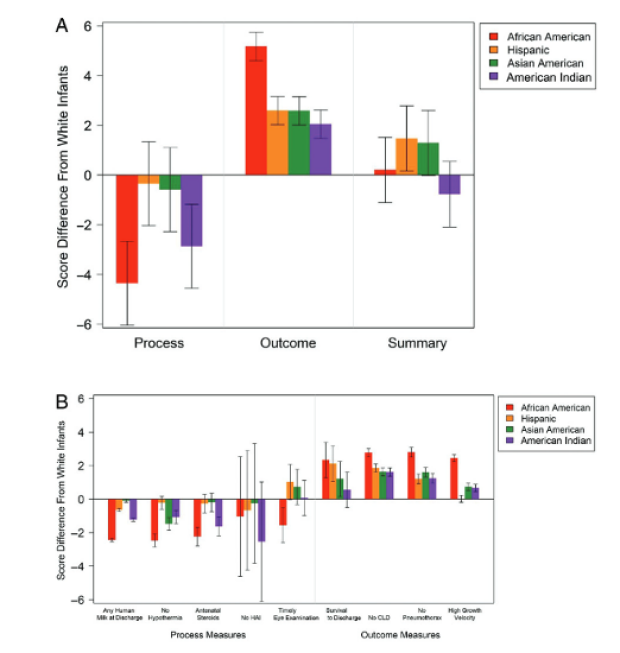
Figure 1. Point estimates and 99% compatibility intervals indicated with error bars for Baby-MONITOR scores by racial and ethnic group, compared with those of white infants. Positive scores indicate that multiracial racial and ethnic groups scored better across NICUs than white infants. A, Process, outcome, and summary Baby-MONITOR scores by race and ethnicity compared with those of white infants across all NICUs. B, Baby-MONITOR measure scores for racial/ethnic groups compared to white infants across all NICUs. CLD, chronic lung disease; HAI, hospital-acquired infection.
Jul July 06 Tue 2021
Profit Lab colleague Daniel Tawfik, MS, MD, collaborated with Dr. Profit and the Duke Center for Healthcare Safety and Quality on a study aiming to evaluate health care workers’ frustration with technology in Journal of Medical Internet Research.
While technological innovations such as the electronic health record (EHR) has led to medical advancement and better quality monitoring, nearly half of physicians believe that they spend too much time on electronic clerical tasks and many believe that the EHR contributes to burnout. One component of burnout related to technology in health care maybe frustration with technology, defined here as an emotional reaction to an obstacle preventing the fulfillment of a need. The study authors set out to quantify the magnitude of health care workers’ (HCWs) frustration with technology and its potential relationship with emotional exhaustion (burnout) and work-life integration (WLI). The authors employed a secondary analysis of the results of the Safety, Communication, Operational Reliability, and Engagement (SCORE) survey administered to Michigan Health and Hospital Association Keystone Center HCWs in 2015. Results of the study indicated that frustration with technology was associated with burnout and that magnitude of frustration with technology varied across and within settings. Six out of seven items from the WLI scale were additionally independently associated with emotional exhaustion. The authors acknowledge that despite the observed correlations between frustration with technology and other WLI items with emotional exhaustion, there is no evidence of a causal relationship.
KEY TAKEAWAY: Frustration with technology and difficulty sleeping were the biggest WLI factors associated with burnout. Addressing frustration with technology and other WLI aspects may reduce level of HCW burnout.
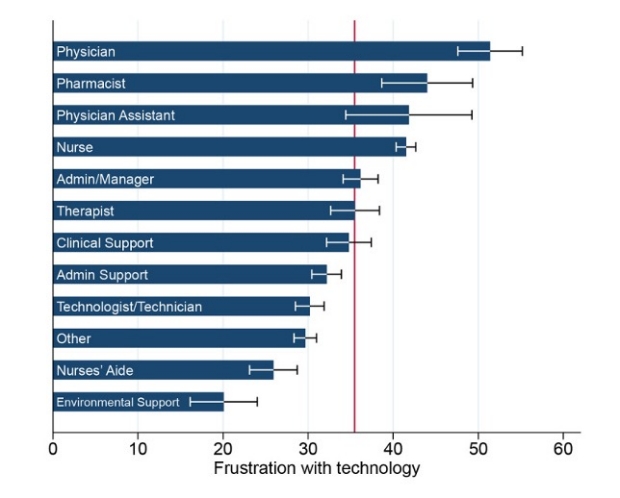
Figure 1. Frustration with technology scores by job position. Data shown as mean values and 95% confidence limits of the mean, with the reference line at a population mean of 35.03.
Jul July 06 Tue 2021
Profit Lab colleague Daniel Tawfik, MS, MD, collaborated with Dr. Profit and the Duke Center for Healthcare Safety and Quality on a study aiming to evaluate health care workers’ frustration with technology in Journal of Medical Internet Research.
While technological innovations such as the electronic health record (EHR) has led to medical advancement and better quality monitoring, nearly half of physicians believe that they spend too much time on electronic clerical tasks and many believe that the EHR contributes to burnout. One component of burnout related to technology in health care maybe frustration with technology, defined here as an emotional reaction to an obstacle preventing the fulfillment of a need. The study authors set out to quantify the magnitude of health care workers’ (HCWs) frustration with technology and its potential relationship with emotional exhaustion (burnout) and work-life integration (WLI). The authors employed a secondary analysis of the results of the Safety, Communication, Operational Reliability, and Engagement (SCORE) survey administered to Michigan Health and Hospital Association Keystone Center HCWs in 2015. Results of the study indicated that frustration with technology was associated with burnout and that magnitude of frustration with technology varied across and within settings. Six out of seven items from the WLI scale were additionally independently associated with emotional exhaustion. The authors acknowledge that despite the observed correlations between frustration with technology and other WLI items with emotional exhaustion, there is no evidence of a causal relationship.
KEY TAKEAWAY: Frustration with technology and difficulty sleeping were the biggest WLI factors associated with burnout. Addressing frustration with technology and other WLI aspects may reduce level of HCW burnout.
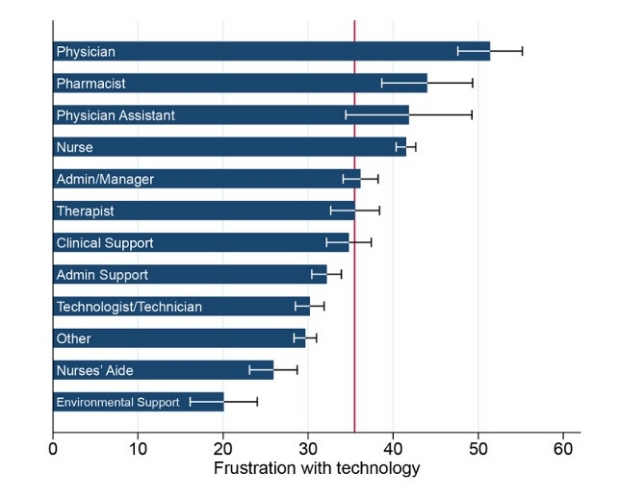
Figure 1. Frustration with technology scores by job position. Data shown as mean values and 95% confidence limits of the mean, with the reference line at a population mean of 35.03.
May May 27 Thu 2021
Dr. Daniel Tawfik and Dr. Profit collaborated with researchers from Stanford and the Duke Center for Healthcare Safety and Quality on a study of work-life integration in physicians in JAMA Network Open.
The research team investigated the personal and professional characteristics associated with work-life integration (WLI) in physicians as well as the factors modifying the association between gender and WLI. The research team surveyed a sample of US physicians from all specialties with the American medical Association Physician Masterfile and oversampled physicians from specialties with lower representation to assure balance across specialty groups. WLI was evaluated using a standard 8-item scale and transformed to a 100 point scale for ease of interpretation. Of all physicians contacted about participation, 4370 provided complete responses. Demographic characteristics of the participants reflected the overall demographics of physicians in the United States. Mean WLI scores were lower in women than in men for overall WLI and 6 of 8 items of the scale. Results of univariate and multivariate analyses indicated that women from all subgroups reported lower WLI scores, although the gender disparity was lower the more hours per week worked. The largest gender disparities were observed among physicians aged 45 to 54 years. The authors suggest that poor reported WLI may adversely impact physicians and families and correlates with increased burnout and warrants systemic change that would empower physicians to strive for better balance between work and home responsibilities.
KEY TAKEAWAY: Lower WLI reported in women, single, >35 years, those who work more hours and call nights indicate a need for systemic change to achieve better integration of work and home responsibilities.
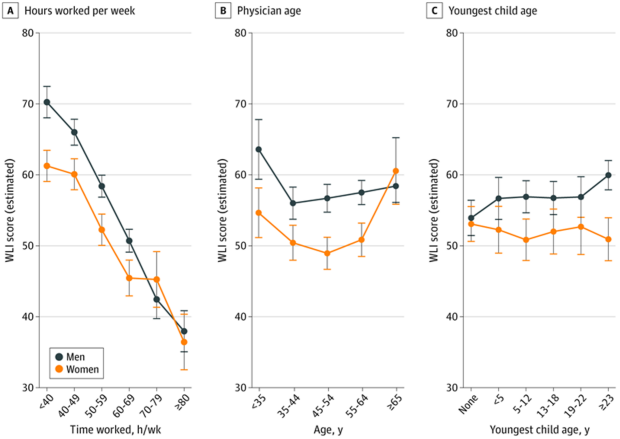
Figure 2. Estimated WLI scores showing the interactions between gender and (A) mean hours worked per week, (B) physician age in years, and (C) age of youngest child in years. Models also adjusted for relationship status and specialty. Error bars denote 95% CIs.
Apr April 13 Tue 2021
Dr. Profit and colleagues from the International Neonatal COVID-19 Consortium published a follow-up survey of COVID-19 preparedness with responses from 145 neonatologists in 58 low and middle-income countries in Journal of Perinatology.
The authors of the study reported distinct differences in national guidance in particular regarding triaging, use of personal protection equipment, viral testing, and visitor policies. Local protocols also tended to deviate from national guidelines. The report highlights how, in the face of a pandemic like COVID-19, rapidly available, consensus-based international, real-time information exchange could better inform local guideline formation and implementation. Diversion of scarce resources such as ventilators and health care workers and the restriction to parent visitation policies could significantly impact quality of care for babies. Dr. Profit and consortium colleagues during the summer conducted a survey of 145 neonatologists in 58 countries, citing the need for better international coordination in development of neonatal guidelines and how quality of NICU care is affected by limited resources.
KEY TAKEAWAY: Many low and middle-income countries face an exacerbation of preexisting resource challenges for neonatal care during the pandemic.
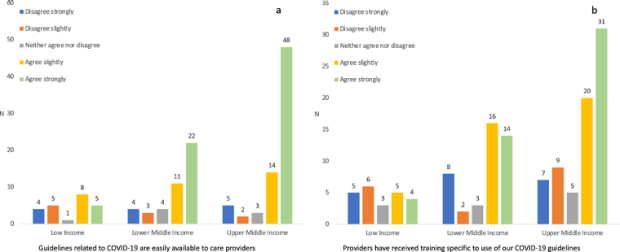
Figure 2. Responses to survey questions. a) “Guidelines related to COVID-19 are easily available to care providers,” and b) “Providers have received training specific to use of our COVID-19 guidelines.”
Mar March 16 Tue 2021
Stanford Neonatology Fellow Dr. Eman Haidari and colleagues from Stanford CMQCC and CPQCC contributed to analysis of a survey of maternal and neonatal health care workers well-being during the COVID-19 pandemic.
The COVID-19 pandemic has been reported to exacerbate health care worker (HCW) burnout and well-being. The authors of this study sought to understand the level of burnout in health care workers during the COVID-19 pandemic with an anonymous electronic survey of maternal and neonatal HCWs, administered during late May – early June of 2020. The brief survey was composed of 13 well-being and patient safety items including a 5-item emotional exhaustion scale. 288 individuals fully completed the survey, with the majority of respondents being nurses and female. Of the 288, 73% reported increased burnout in their coworkers and 66% reported their own increased emotional exhaustion in the month prior. A majority of respondents reported difficulty with work-life balance and nearly half felt that the efforts of their institutions to counteract the effects were inadequate.
KEY TAKEAWAY: Although the long-term impact of the COVID-19 pandemic on HCWs is unknown at this time, the reported high levels of burnout and negative perceptions of well-being and care culture indicate a need for stronger institutional support and intervention to mitigate potential adverse outcomes for HCW well-being.
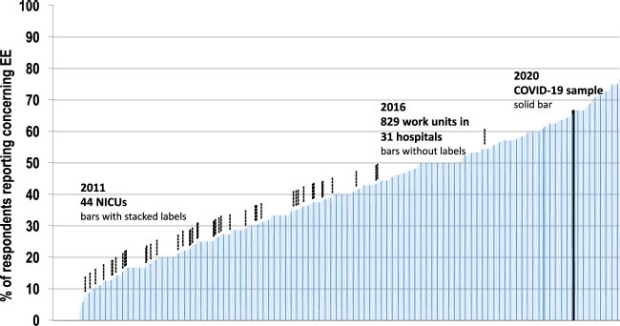
Figure 3. Comparison of burnout (emotional exhaustion) in current sample with prior NICU and adult samples. Each bar shows % respondents reporting moderate to severe burnout in either the current sample, a NICU, or a hospital work setting. COVID-19 June, 2020 sample (solid bar; mean % reporting emotional exhaustion was 66%). Sample from 44 California NICUs in 2011 (stacked bar labeled; mean % reporting emotional exhaustion was 26%) used a 4-item scale to which we subsequently added an additional item for improved construct validity. Unit level correlation between scales exceeds 0.98. Sample from 829 work settings in 31 hospitals in Michigan in 2016 (no label; mean % reporting emotional exhaustion was 40%) responded to the 5-item scale.
Jan January 23 Sat 2021
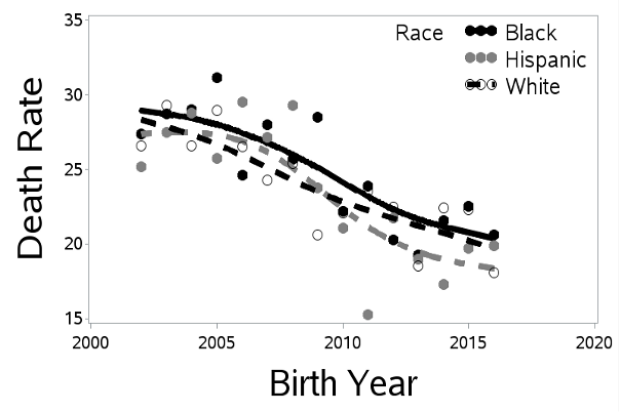
Dr. Profit and colleagues published an article describing the gaps in knowledge and barriers to research for more mature, higher birthweight newborns representing 80% of NICU admissions in Seminars in Perinatology.
While inpatient NICU care is seen as the care typically provided to very low birthweight and preterm infants, roughly 80% of NICU admissions involve infants ³34 weeks. We identified wide variation in NICU admission rates, length of stay, and proportion of high acuity infants in NICUs around the United States for infants in this population. We conclude that there is a need for birth population based studies and population specific data elements to better understand optimal management of the more mature NICU newborn.
KEY TAKEAWAY: The more mature newborns constitute a large, heterogenous population and receive a large proportion of the care we provide in NICUs. We have identified some important knowledge gaps and obstacles that need to be addressed including expanded data collection, perspectives from families and public oversight, and sharing of information across medical entities and between public and private systems to serve the best interests of the full range of babies who depend on us for their wellbeing (Fig. 1).
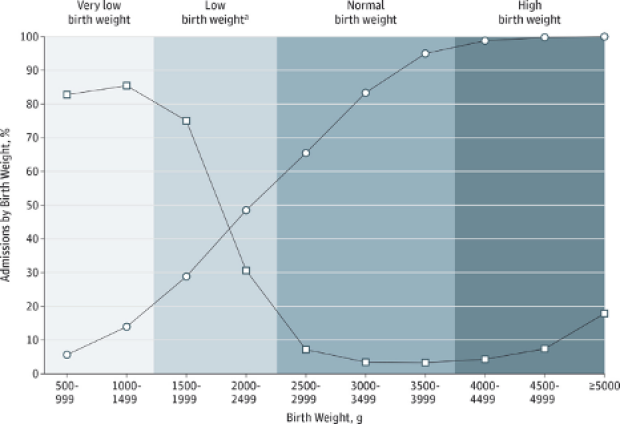
Figure 1. Level III and IV NICU admissions by Birth Weight for the 2012 US Birth Cohort. Adapted from Harrison 2015. The admission rate uses the total 2012 birth cohort as the denominator, whereas the denominator for the cumulative percentage of the total neonatal intensive care unit (NICU) admissions represents only US newborns admitted to a NICU. Circle: cumulative percentage of total NICU admissions. Square: Admission rate. “Indicates low birthweight exclusive of very low-birthweight designation.” Reprinted with Permission.