The ProfitLab

Welcome
Under the direction of Dr. Jochen Profit, our lab focuses on optimizing quality of healthcare delivery to the most vulnerable patients, infants in the neonatal intensive care unit (NICU) setting, with a strong focus on health equity and care culture. Our research is community participatory and transdisciplinary, including patient and family advocates, clinicians, psychologists, sociologists, economists, health services researchers, biostatisticians, computer scientists, and others. We employ a variety of methods, ranging from randomized clinical trials to qualitative analyses. One of our great strengths is our ability to query linked multi-level data from the California Perinatal Quality Care Collaborative (CPQCC), a multi-stakeholder population based network of ~140 NICUs. While our epidemiological work has brought to light opportunities for improvements in health equity in NICU care and quality optimization, we pride ourselves on a strong solution-focused vision. For example, we established a health equity Taskforce for the CPQCC, which is translating our findings into quality improvement solutions with routine measurement of equity in care, promotion of family-centered care, and a focus on building improvement capacity at safety net hospitals. Our work in these areas leads the field and has been recognized nationally and internationally.
We are housed within the California Perinatal Quality Care Collaborative, an organization committed to improving the quality of care for the state's mothers and most vulnerable infants.
Jochen Profit,
MD, MPH
Professor of Pediatrics
Chief Quality Officer
California Perinatal Quality Care Collaborative
(650) 725-9933
profit@stanford.edu
Administrative Assistant
Gabriela Luna-Victoria
glv@stanford.edu
In Brief | Lab News
Jan January 23 Sat 2021
Dr. Profit and colleagues published an article describing the gaps in knowledge and barriers to research for more mature, higher birthweight newborns representing 80% of NICU admissions in Seminars in Perinatology.
While inpatient NICU care is seen as the care typically provided to very low birthweight and preterm infants, roughly 80% of NICU admissions involve infants ³34 weeks. We identified wide variation in NICU admission rates, length of stay, and proportion of high acuity infants in NICUs around the United States for infants in this population. We conclude that there is a need for birth population based studies and population specific data elements to better understand optimal management of the more mature NICU newborn.
KEY TAKEAWAY: The more mature newborns constitute a large, heterogenous population and receive a large proportion of the care we provide in NICUs. We have identified some important knowledge gaps and obstacles that need to be addressed including expanded data collection, perspectives from families and public oversight, and sharing of information across medical entities and between public and private systems to serve the best interests of the full range of babies who depend on us for their wellbeing (Fig. 1).
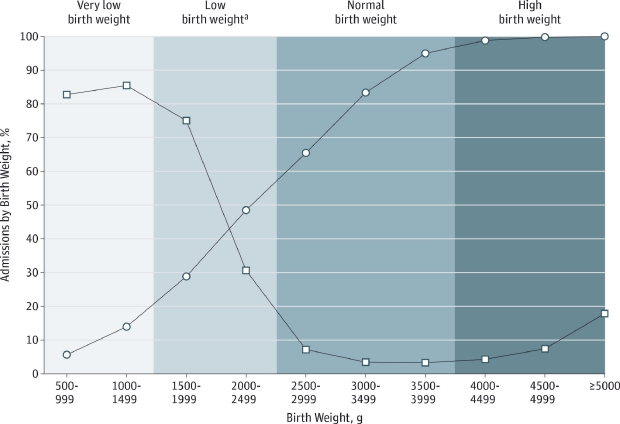
Fig 1. Level III and IV NICU admissions by Birth Weight for the 2012 US Birth Cohort. Adapted from Harrison 2015. The admission rate uses the total 2012 birth cohort as the denominator, whereas the denominator for the cumulative percentage of the total neonatal intensive care unit (NICU) admissions represents only US newborns admitted to a NICU. Circle: cumulative percentage of total NICU admissions. Square: Admission rate. “Indicates low birthweight exclusive of very low-birthweight designation.” Reprinted with Permission.
Dec December 05 Sat 2020
We collaborated with Duke Center for Healthcare Safety and Quality collaborators Drs. J. Bryan Sexton and Kathryn C. Adair on a study investigating the relationship between health care worker assessments of good institutional support for “second victims” and organizational safety culture and well-being in The Joint Commission Journal on Quality and Patient Safety.
Our cross-sectional study looked at 2016 data collected from 10,627 health care workers (HCWs) as part of the Safety, Communication, Operational Reliability, and Engagement (SCORE) survey. The percentage of HCWs who reported being aware of at least one colleague (second victim) in their work setting who has been emotionally traumatized by an unanticipated clinical event was 36.3%. We found that perceived institutional support for second victims, based on a single item metric, was significantly associated with better safety culture and lower emotional exhaustion.
KEY TAKEAWAY: Good institutional support for “second victims” predicts better safety culture and well-being in a large sample of health care workers.
Funding: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01 HD084679).