Research
Regeneration of nerve tissue and blood supply after nerve injury
Nerve injury, whether the result of trauma or surgical transection in preparation for repair, has long been viewed differently than other soft tissue wounds. However, like all wounds, nerve injury requires a regenerative response that restores the structure and blood supply of the injured tissue.
Using a microsurgical model of facial nerve injury in the mouse that we developed, our research explores the molecular pathways that drive nerve tissue regeneration after injury. We are particularly intrigued by the ways that nerve connective tissue, or mesenchyme, responds to injury. Our prior work has highlighted the role of the Hedgehog pathway in mediating this response to nerve injury.


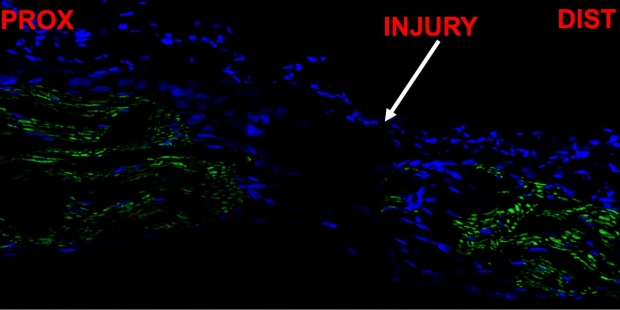
This image, featured on the cover of Experimental Neurology, shows endoneurial fibroblasts (marked in red) repopulating the injured facial nerve. Our subsequent work has shown that these endoneurial fibroblasts participate in repair of the injured nerve and likely express angiogenic factors that help to restore the blood supply of the nerve.
Improving Nerve Regeneration After Injury
Based on our prior work, we now employ targeted small molecules to modulate key signaling pathways as a means of increasing the rate of recovery after facial nerve transection injury.

Small molecules applied during the time of nerve injury and recovery may hasten the recovery of the nerve. The top image shows a facial nerve two weeks after transection injury, with the mouse treated with a small molecule before and after nerve injury. A mouse treated with vehicle is shown below, also two weeks after facial nerve transection injury.
Surgical Innovation at the Stanford Facial Nerve Center
Our scientific discoveries in the lab improve the ways in which we treat our patients. Our work on facial nerve regeneration in the mouse model has informed the development of new microsurgical techniques for the treatment of facial paralysis.
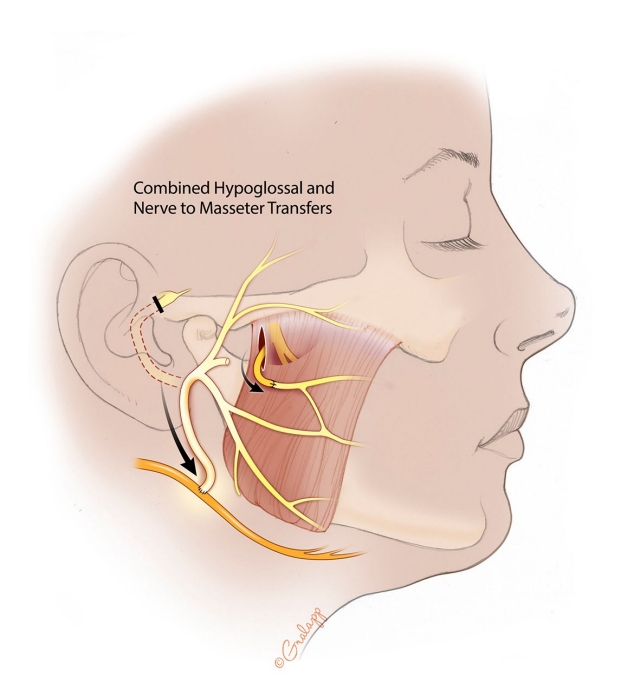
The Dual Nerve Transfer for facial reanimation describes the combination of a masseteric nerve transfer with a simultaneous end-to-side nerve transfer of the proximal facial nerve to the hypoglossal nerve.
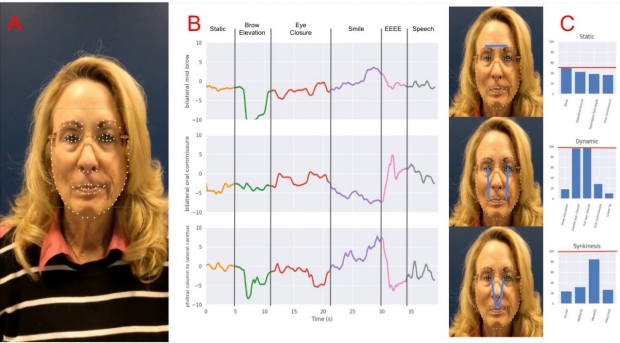
Dynamic Analysis of Facial Paralysis
Unilateral facial palsy is surprisingly common, affecting almost 100,000 Americans per year; Bell’s palsy accounts for approximately half of all cases. The Stanford Nerve Center uses the eFACE, a validated clinician-scored metric that is employed to rate a patient’s facial palsy based on a series of standardized facial exercises.
Since facial palsy affects both symmetry of the face in repose and during facial movement, the analysis of still frames and photographs is not optimal for diagnosis and analysis. However, clinician scoring entails time-intensive watching and rewatching of videos to score facial palsy using metrics such as the eFACE. The goal is to create an automated, video-based method of scoring facial symmetry in real-time using computer vision and deep learning.