Multidisciplinary Head & Neck Cancer Care
Head & Neck Surgery
We are the pioneers of major scientific breakthroughs
- Organ preservation approaches to head and neck cancer.
- New drugs for head and neck squamous cell carcinoma (HNSCC) and extending uses of existing drugs to HNSCC and nasopharyngeal carcinoma (NPC).
- Advanced radiation therapy techniques that limit toxicity and improve outcomes.
- Minimally Invasive and Robotic Surgery
- Stem cell work that extends the findings of the first paper, demonstrating the existence of “cancer stem cells” in HNSCC by researchers from Stanford and Michigan in 2007; and a 2009 Stanford study establishing that stem cell properties of patients’ malignancies correlate with prognosis. This work led to subsequent stem cell papers in 2011 and 2012.
- Normal tissue stem cell studies to identify salivary gland stem cells and to manipulate them for preservation and/or restoration of salivary gland function from radiation damage.
- HNOP’s breadth of research studies and protocols including treatment of intermediate and advanced disease as well as hypoxia imaging.
Our Innovations
- Creation of the first head and neck multidisciplinary tumor patient conference (tumor board; 1976) in the U.S.
- Introduction of the first use of chemotherapy with irradiation for head and neck squamous cell carcinoma (HNSCC), which is the basis of organ-preservation chemoradiation in the U.S.
- Close working relationships with:
- Neurosurgery, Interventional Radiology, and Neuroradiology,which are critical for complex open and endonasal endoscopic skull base surgery.
- Endocrinology in the treatment of thyroid cancer.
- Dermatology in the treatment of advanced skin cancers.
- Innovative research by physicians now at Stanford that demonstrates the utility of the FDA-approved Mobetron for intraoperative radiation therapy.
- Contributing research in a Phase II trial of immunotherapy in intermediate and advanced surgically-treated HNSCC. A Phase III trial is now planned.
- Leadership in the head and neck disease site committee of the Radiation Therapy Oncology Group to develop new nation-wide clinical trials in head and neck cancer.
- Biomarker studies to identify novel circulating biomarkers for prognostication and post-treatment surveillance in head and neck cancer.
- Strong links to developmental therapeutics such as the advancement of new drugs to treat cancer.
- Provision of a full range of treatment options that include minimally invasive surgery, robotic surgery, stereotactic radiosurgery such as CyberKnife, microvascular reconstruction, intraoperative radiation therapy (IORT), and new chemotherapy trials.
What is Head & Neck Cancer?
Head and neck cancer is a term that can include the broad array of tumors which may arise in this anatomically diverse region of the human body. Most often, the term head and neck cancer refers to tumors that arise from “squamous” cells that line the moist, mucosal surfaces of the mouth and throat. In fact, 95% of head and neck tumors are squamous cell carcinoma.
Tumors of the thyroid, salivary, and parathyroid glands, as well as cancers of the brain, nose and paranasal sinuses, esophagus, and eye, are not usually categorized as head and neck cancer. Furthermore, tumors of the skin, muscle and bone arising in the head and neck are also typically not included in this term.
Head and neck cancer is then further classified by its location within the mouth and throat:
Oral cavity
The lips, the oral tongue” (the forward two-thirds or front part of the tongue), the gums lining the upper and lower jaws, as well as the lining inside the cheek. The area known as the floor of the mouth is a mobile area between the lower jaw and gum and the oral tongue. The roof of the mouth or “hard palate” is also included as part of the oral cavity. Finally, a small triangulated area of mucosa or gum lining the area behind the last wisdom tooth is called the“retromolar trigone” and is also part of the oral cavity.
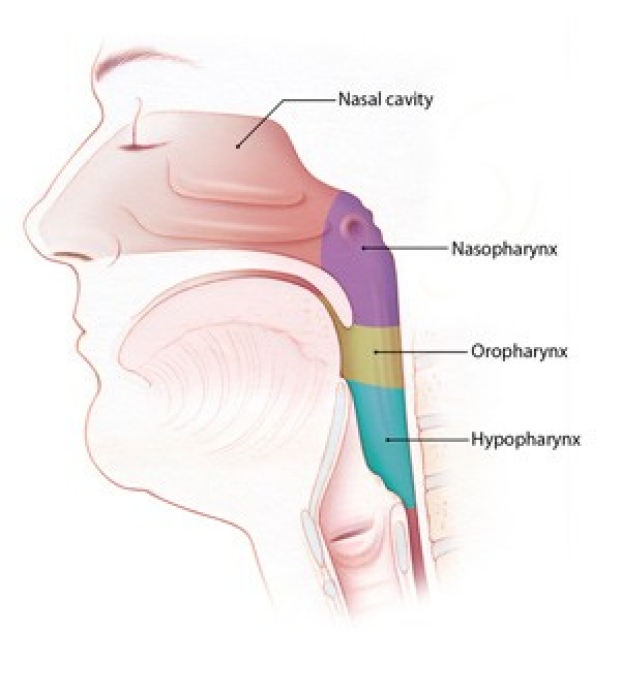
Pharynx
In medical terminology, the throat is known as the pharynx. In fact, the pharynx is supple tube or funnel that connects both the nose and mouth to the swallowing tube or esophagus. The pharynx is composed of three parts: the nasopharynx (the area just behind the nose); the oropharynx (behind the oral cavity and in the back of the mouth], and the hypopharynx, which surrounds the voice box and leads into the esophagus.
The larynx critical not only for the production of speech, but also breathing and swallowing. The “supraglottic” larynx has a valve called the epiglottis, which covers the larynx during swallowing to prevent “aspiration” of food into the lungs.

Treatments
HNOP offers multi-disciplinary, collaborative and integrated evaluation and care for patients with head and neck cancers.
Minimally invasive or endoscopic head and neck surgery (eHNS) is a dynamic new approach that allows surgeons to remove tumors with use of a specialized endocopes and cameras without external incisions and usually with little or no change in speech, appearance, and swallowing function.
An endoscope is a long, thin tube with special lighting and a narrow lens through which the surgeon can view organs and tissue inside of the body. For throat cancers, the surgeon inserts the endoscope through the patient’s mouth, and a microscope provides an excellent image of the tumor. Using very precise, state-of-the-art surgical instruments that are also inserted through the mouth, the surgeon can perform the operation without an external incision.
eHNS has several advantages in many cases. Some of these advantages are:
- Reduced risk of blood loss
- Lower pain levels
- Fewer days spent in the hospital
- Quicker return to a normal diet and faster recovery time
- Less scarring, with improved cosmetic appearance
In some cases of throat cancer, eHNS may reduce or even eliminate the need for chemotherapy and radiation therapy.
At Stanford, your team of surgeons, oncologists, and radiologists will work together to determine the best course of action for you. The goal with eHNS is always the same: to eliminate the cancer while minimizing the risks and recovery time associated with traditional cancer care.
Chemotherapy or radiation therapy may still be necessary after eHNS. When chemotherapy and radiation therapy cannot be avoided through surgery, eHNS may still hold advantages for patients. Faster recovery after eHNS means patients can usually begin chemotherapy and radiation therapy earlier. And the smaller incisions with eHNS heal more quickly than larger incisions and are less likely to become infected.
Two types of eHNS, transoral robotic surgery (TORS) and transoral laser CO2microsurgery (TLM), have revolutionized the treatment for throat cancer.
Robotic surgery uses state-of-the-art technology that allows surgeons to safely remove certain thyroid tumors through discrete incisions several inches from the neck. Because no incision is made in the neck, the patient avoids a neck scar.
The da Vinci ® surgical system is a highly sophisticated computerized system that is used for robotic thyroid surgery. The surgeon cuts a 1-inch to 2-inch incision in the folds of skin under the patient’s arm and inserts the da Vinci ® system’s robotic arms, which have been customized to resemble standard surgical instruments. The surgeon guides the robotic arms underneath the skin toward the thyroid gland.
The surgeon views the surgical field on a 3-D high-definition screen, magnified up to 10 times. The skilled surgeons at Stanford Medicine control the da Vinci ® system’s robotic arms as one might control conventional surgery. The instruments on the robotic arms can move with seven degrees of movement and rotate 540 degrees, giving the surgeon the ability to manipulate delicate tissues with precision.
Robotic thyroidectomy is not available for all thyroid tumors. If your thyroid tumor is less than 3 cm in size and is likely to be benign (non-cancerous), then robotic surgery may be an option. Your surgeons will help you decide the best approach for you.
Clinical Trials
No trials match your search ""