Microtia
What is Microtia?
Microtia is a congenital deformity of the outer ear where the ear does not fully develop during the first trimester of pregnancy. The word “microtia” comes from the Latin words “micro” and “otia”, meaning “little ear.” Microtia ears can vary in appearance, but are usually smaller in size, often only consisting of a tiny peanut-shaped lobe. Microtia occurs about 1 in 5,000 births, though rates can vary depending on ethnic background. It is unilateral in above 90% of cases, and tends to involve the right ear more commonly, and also more common in males. Microtia describes the outer ear, and is often associated with absence of the ear canal (called canal atresia or aural atresia). The ear canal can also be present or extremely narrow (canal stenosis).
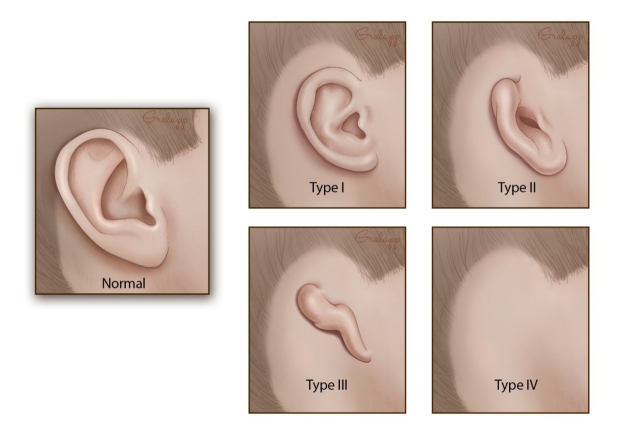
There are four grades of Microtia:
| Grade 1 | The ear is smaller than normal but the key features of the normal ear are present, though they may have minor alterations in shape or form. |
| Grade 2 | Some of the features of the ear are missing, though usually there is still a lobule and a remnant of helix and antihelix. Grade 2 microtia is sometimes called “conchal type microtia.” The ear canals may be present, though frequently are very narrow (canal stenosis). |
| Grade 3 | This is the most common type of microtia, in which the only feature remaining is a small peanut-shaped remnant ear lobe. Grade 3 microtia is sometimes called “lobular type microtia.” The ear canal is usually completely absent (aural atresia). |
| Grade 4 | Complete absence of the external ear without any remnant. This is called “anotia”, and actually rarely seen. |
Is microtia genetically inherited?
In most cases, no. In 95% of children with microtia, there is no family history of microtia or other major ear anomalies in either the paternal or maternal side of the family. In the majority of cases, microtia appears to be a randomly occurring event or anomaly that happens during early development of the embryo. One child may be born with microtia where his/her twin sibling may not show any signs of having microtia.
In approximately 5% of cases, there can be a genetic etiology, with microtia present in multiple family members. Sometimes an aunt, uncle, grandparent, or cousin may have had microtia. Microtia can skip family generations, and one family member may have right ear affected while another has the left ear affected. One family member may even have bilateral microtia when every one else only had unilateral microtia. It has been estimated that if you have a child with microtia, there can be an increased 5% risk of having another child with microtia. Likewise, the risk of a child with microtia eventually having a child of his/her own with microtia has been estimated to be 5%.
What other medical problems are associated with microtia?
Most patients with microtia have no other significant medical problems aside from the ear. Approximately 50% have underdeveloped bony and soft tissues on the involved side of the face (hemifacial microsomia). Up to 15% can have varying degrees (from slight to more severe) of facial nerve weakness. Other general abnormalities such as cleft lip or palate, cardiac, or urological problems are infrequently encountered.
Microtia is sometimes associated with other craniofacial syndromes, such as Treacher Collins Syndrome and Goldenhar Syndrome (oculoauriculovertebral dysplasia).
Microtia patients often have canal atresia or stenosis. Patients with canal atresia or stenosis usually fail the newborn hearing screening, and must be referred to a pediatric audiologist for further diagnostic evaluation as well as discussion of auditory rehabilitative options.
What are some possible causes of microtia?
In most cases it is not known the precise cause of microtia. As microtia is a rare condition, it is not often found on prenatal ultrasound. Possible etiologies include:
- It is possible that blockage to the blood supply due to pressure from positioning of the fetus against the inside of the mother or from the umbilical cord during the 1st trimester can cause under-development of the external ear. This would be analogous to the situation seen sometimes when children are born with under-developed limbs because the umbilical cord was wrapped around the limb resulting in cessation of development.
- A drop in oxygen levels during pregnancy within the 1st trimester may cause the ear to cease in development. During the 1st trimester, the heart, kidneys, and ears develop at the same time. Sometimes anomalies are seen in all three of these systems due to the organs being affected simultaneously.
- Excessive drugs and alcohol during pregnancy can possibly cause microtia and ear canal atresia, although this is a rare cause. Usually, drugs and alcohol also cause other significant medical issues and microtia is just one of many effects. Fetal Alcohol Syndrome has been known to cause microtia in some babies. Microtia can also result from taking Accutane (isotretinoin) and methamphetamines during pregnancy.
How do we evaluate microtia?
After birth, once the microtia is recognized, many children may undergo an ultrasound evaluation of their kidneys to check for normal anatomy. A hearing screening is then done after birth, and further evaluations of the hearing will be done with an Audiologist to check for the degree of hearing loss. If there are any other abnormalities noted at birth, a consultation with a geneticist may be valuable. A consultation with an Ear, Nose and Throat doctor is important to evaluate the severity of microtia, establish the presence or absence of the ear canal, and discuss reconstruction options and hearing amplification options. If microtia is part of a craniofacial syndrome (e.g. Treacher Collins Syndrome), the child may also be evaluated by a craniofacial team of doctors, therapists and support staff.
Should we have a CT Scan?
For the purposes of looking at the middle and inner ear of the affected microtia ear, it is almost never useful to obtain a CT scan when the child is young. A newborn child or child of a younger age is more susceptible to the radiation exposure emitted from the CT scan, and this risk decreases with age. Also, many of the tiny structures that we need to visualize may not be well defined on the CT scan until the skull and temporal bone is closer to adult size. Most canal atresia reconstruction surgeons would like to wait to get the CT until a time very close to the intended canal reconstruction, which must be done after the child has completed reconstruction of the external ear with rib cartilage graft (and this is often not until 9 or 10 years of age).
How is microtia treated?
The most difficult thing for many parents is to know that reconstruction of the outer ear malformation cannot be done right after birth. Parents are faced with how they and the child copes with the abnormality until the reconstruction can be done, and at times this can be difficult. Talking to your family, friends and to your child about the issues can really help you and your family not feel embarrassed or ashamed.
What are reconstructive options for microtia?
In the 2nd stage, incisions are made behind the ear to release the ear from the scalp skin, and the cartilage framework is lifted up to give it adequate projection. A skin graft is then used to help cover the backside of the newly lifted ear. Sometimes, additional minor stages are performed to improve the shape of the ear, the appearance of scars, or elevate the ear even further.
A common technique used in the US is the Brent technique, which is a 3-stage technique. The Nagata technique, similar to the Firmin technique, is also a 2-stage technique. Although some surgeons consider doing rib cartilage graft reconstruction as early as 5 to 6 years of age, a much better and more detailed 3-dimensional reconstruction can be achieved at 8 to 10 years of age, when there is a thicker, more robust rib cartilage to be harvested from the chest.
If reconstruction of ear canal atresia is also desired, and if your child is a candidate for this surgery, it must be performed after the external ear has been completed, because the 1st stage of rib cartilage graft implantation depends upon the skin flap overlying the cartilage to have good blood supply that has not been compromised by any previous surgical incisions in the region.
Advantages of the rib graft reconstruction:
The main advantage of the rib graft is that the tissue used for the reconstruction is from the child’s own body, decreasing the risk that the body rejects the implant. The newly constructed ear is living tissue created from the patient’s own cartilage, and will feel pain, experience bleeding, and heal spontaneously with injuries. Rib cartilage is proven to resist trauma and contact sports are permitted without extra protection or restriction. Ears constructed by this method retain their form and have withstood the test of time and should last a lifetime.
Disadvantages of the rib graft reconstruction:
The disadvantages include pain from the rib harvest site at the time of the initial surgery that resolves when the child is healed. There will be a scar and a risk of a small deformity of chest at the donor site. Reconstructed rib graft ears will be slightly stiffer than the biological ear since the rib graft is thicker and stronger than ear cartilage. At times, the initial healing of the reconstructed graft can be unpredictable.
2. Medpor Graft Surgical Reconstruction
Medpor graft surgery utilizes a synthetic pre-made porous polyethylene framework, eliminating the need for harvesting rib cartilage. The implant is covered with tissue from the scalp, called temporalis muscle fascia, and placed under the child’s skin. This can be achieved with just one stage and can be performed as early as 3 years of age.
If reconstruction of ear canal atresia is also desired, and if your child is a candidate for this surgery, it can be performed before the external reconstruction utilizing Medpor. There are some surgeons that will actually do the ear canal and external ear Medpor reconstructions simultaneously in one single surgery/anesthesia.
Advantages of MedPor grafts
The advantage of this technique is that it requires only one stage and theoretically can be done at an earlier age in comparison to rib cartilage reconstruction. It also does not require a donor site and eliminates the pain and healing from this site. The MedPor implant typically has less variability in the cosmetic outcome.
Disadvantages of MedPor graft
This technique is a technically challenging surgery that most microtia surgeons do not perform. It requires a well-vascularized temporalis muscle fascia flap for the implant to successfully heal, and even then, the Medpor implant never becomes a living part of the body like a cartilage graft. Even minor trauma occurring in the future can cause an opening, increasing the risk of infections, exposing part of the Medpor implant, and ultimately resulting in complete extrusion of the entire implant and complete loss of the ear. One other problem with Medpor reconstructions is that they are covered completely with insensate skin graft, and without protective sensation, they are more likely to sustain trauma un-noticed by the patient, leading to potential extrusion and loss of implant. This risk is life-long for the patient. At this stage, there is less than 20 years long term follow-up with Medpor ears and it is not known how long they can last without failing. Due to these significant concerns, we do not perform Medpor reconstructions at Stanford.
Since there is a concern about surgical trauma causing exposure and loss of Medpor implant, it is generally favored for patients getting Medpor to have their ear canal reconstructions done before external ear reconstruction.
3. Prosthetics
With a good anaplastologist (the specialist who creates the prosthetic), a prosthetic ear can be made to look very real. They can be worn by either adhesive or by being attached to an implanted anchor system to allows a secure fit (which does require a minor surgery to place).
Advantages of ear prosthetics
An ear prosthetic can look cosmetically excellent and mirror the opposite ear. They are made with materials that feel close to skin, and can be an excellent option if other options have failed. Prosthetics attached with an implanted abutment still allow for patients to swim and bathe with a prosthetic. It is a much less painful surgery and can be done in one stage.
Disadvantages of ear prosthetics
Many people have a difficult time coping with the idea of a prosthetic that comes on and off in comparison to a reconstruction that is formally part of the body. Some patients have difficulty with medical grade glue or an implanted anchor system. The implanted anchor can have a risk of a skin infection around the anchor. The prostheses do wear down over time and need to be replaced, and can sometimes can fall off.
4. The Do Nothing Option
Some individuals opt to not have any reconstruction and to just leave the microtia ear the way it is. Some have adjusted to it, sometimes keeping their hair long so the deformity is not immediately obvious to strangers meeting them for the first time. It is absolutely fine to do nothing. Families that are uncomfortable with the reconstructive options do not have to rush into the decision, because if they decide later when the child is older, the surgery is actually easier because there is more cartilage graft available to make a detailed framework. An older child may be more mature to deal with surgery and the recovery from surgery. Most patients who do complete their reconstructions are very satisfied, and less self conscious when meeting people for the first time. As microtia surgeons, we know we have succeeded when patients come into their clinic visit with their hair cut very short, or their hair tied back in a pony tail or bun to show off their new ear.
1. Rib Cartilage Graft Surgical Reconstruction
This is a reliable reconstruction technique that has been around since the 1920’s. Depending on the exact technique used, this technique usually involves 2 to 4 separate surgeries done under anesthesia separated in time by several months to allow for healing between each stage.
Dr. Kay Chang and Dr Mai Thy Truong, the ear reconstructive surgeons at Stanford Medicine, use the Firmin technique, which is a 2-stage technique.
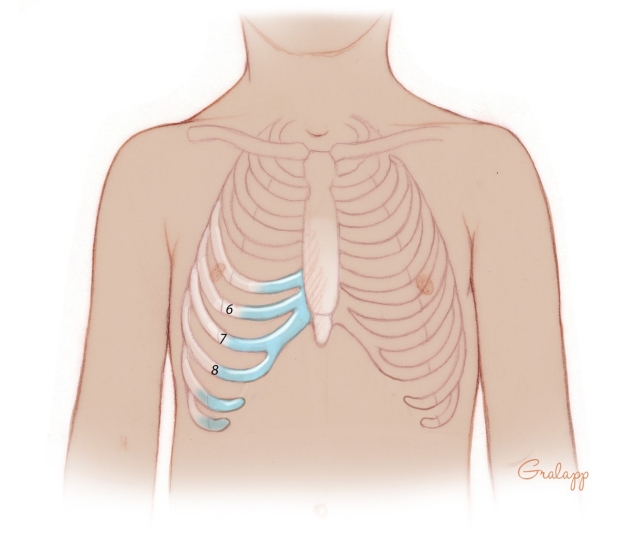
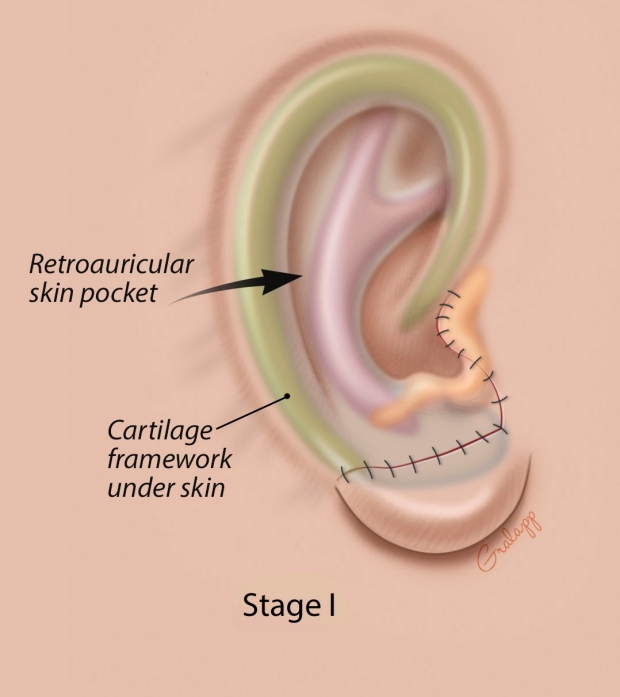
The 1st stage involves harvesting rib cartilage from the chest, and then carefully sculpting the harvested rib cartilage into a framework that is shaped like an ear. This framework is implanted in a skin pocket underneath the scalp on the skull where the new ear will be located. Suction drains are then placed with the implanted rib to create a vacuum that allows the overlying skin to tightly coapt to the framework and allow the detail of the sculpted ear to show thorough. Patients will stay in the hospital for 3 to 5 days until the drains can be removed. The newly created cartilage framework becomes part of the patient’s live tissue, and is incorporated after 3 to 4 months to allow the 2nd stage to be performed.
Stage 1
(click to enlarge)


At what age can microtia be repaired? Can I have my child’s repair done earlier?
As described above, it is not until 8 to 10 years of age that most children have thick and robust enough cartilage to produce a good detailed 3-dimensional auricular framework. It is also easier to actually harvest the graft in a larger child while avoiding creating a deformity of the chest wall. Finally there is a strong psychological reason for waiting. The child with microtia is neither concerned about the problem nor very cooperative before 8 to 10 years of age. This makes postoperative care very difficult on the child and all those involved in their care. We feel that it is important for the child to be old enough to understand and personally “consent” to having the surgery. Even though some surgeons have started surgery in children as young as 5 or 6 years of age, we rarely encounter children requesting surgery at these ages but we frequently encounter parents requesting surgery on their children well before this. Having some patience, and waiting for the child to be physically larger and psychologically more mature results in a far better permanent outcome. The advantages of waiting until a child is older allows for:
- best symmetry in size with the opposite ear after complete growth
- best symmetry in location of the ear in comparison to the opposite ear allowing for growth of the face and jaw
- the presence of a larger more robust cartilage graft from the rib
- a more mature child who can consent and be an active participant in the decision for surgery and in the recovery period.
Treating the Hearing Defect
Most children with microtia have some hearing on that side that is impacted by absence of the ear canal and middle ear structures to allow sound to reach the inner ear. It is important to have close audiological follow up to check for the hearing impact. There are several options for hearing amplification when the inner ear structures are functioning.
- Bone anchored hearing devices
- Ear canal and middle ear reconstructive surgery
Cochlear implants are devices with an electrode that gets inserted into the inner ear for children who are deaf and have no functioning inner ear, which is generally not the case with kids with microtia.
What are the long-term effects of microtia on my child?
The cosmetic effect of having microtia is different for every child and every family. The good news is that most children with microtia grow up to have happy and productive lives. We encourage you and your family to have open discussions about it, and there can be a positive outlook knowing that there are treatments options available if you so choose. Often we find that a child’s feelings about themselves mirror their parents or their family’s feelings.
The hearing effects of microtia: There are concerns that children who do not hear from both ears equally have some disadvantage in learning and language. That is not to say that children with one hearing ear do not grow up to be active and intelligent. However, in school and in noisy environments, there may be a disadvantage to having hearing loss in one ear, so we encourage exploring hearing amplification or surgical reconstructive options.
MAKE AN APPOINTMENT
Pediatric Otology
(650) 724-4800