Eustachian Tube Dysfunction
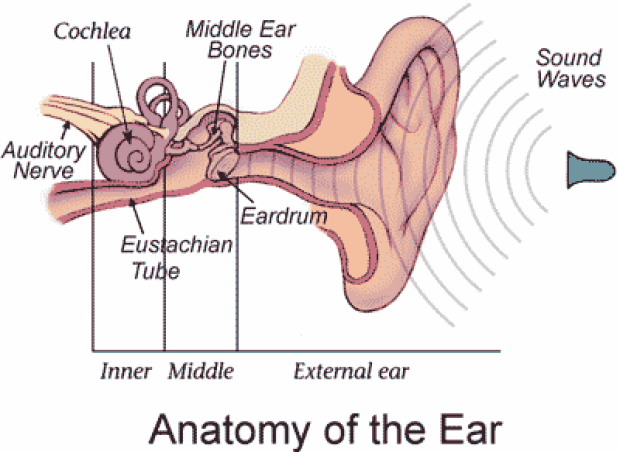
The ear is divided into three parts: the external ear includes the visible part of the ear (the pinna) and the ear canal; the middle ear is the air-filled space behind the eardrum that contains the three middle ear bones (the ossicles); and the inner ear contains the sensory organs of hearing (cochlea) and balance (semicircular canals).
The Eustachian tube is a narrow tube that connects the middle ear to the back of the nose. Normally, the Eustachian tube opens with every swallow or yawn to act as a pressure-equalizing valve for the middle ear. It also serves to drain the mucus produced by the lining of the middle ear.
Blockage of the Eustachian tube isolates the middle ear space from the outside environment. The lining of the middle ear absorbs the trapped air and creates a negative pressure that pulls the eardrum inward. The eardrum is thin and pliable, like plastic wrap, and is densely innervated. When it becomes stretched inward, patients often experience pain, pressure, and hearing loss. Long-term blockage of the Eustachian tube leads to the accumulation of fluid in the middle ear space that further increases the pressure and hearing loss. This is called serous otitis media. Should bacteria contaminate this fluid, a middle ear infection may result, called acute otitis media.
Chronic blockage of the Eustachian tube is called Eustachian tube dysfunction. This can occur when the lining of the nose becomes irritated and inflamed, narrowing the Eustachian tube opening or its passageway. Illnesses like the common cold or influenza are often to blame. Pollution and cigarette smoke can also cause Eustachian tube dysfunction. In many areas of the country, nasal allergy (allergic rhinitis) is the major cause of Eustachian tube dysfunction. For reasons which are unclear, the incidence of allergies is increasing in the United States. Obesity can also predispose a patient to Eustachian tube dysfunction because of excess fatty deposits around the passageway of the Eustachian tube. Rarely, Eustachian tube blockage may be the sign of a more serious problem such as nasal polyps, a cleft palate, or a skull base tumor.
Young children (especially ages 1 to 6 years) are at particular risk for Eustachian tube dysfunction, serous otitis media, and acute otitis media because they have very narrow Eustachian tubes. Also, they may have adenoid enlargement that can block the opening of the Eustachian tube. Since children in daycare are highly prone to getting upper respiratory tract infections, they tend to get more ear infections compared to children that are cared for at home.
Interestingly, the anatomy of the Eustachian tube in infants and young children is different than in adults. It runs horizontally, rather than sloping downward from the middle ear. Thus, bottle-feeding should be performed with the infants head elevated, in order to reduce the risk of milk entering the middle ear space. The horizontal course of the Eustachian tube also permits easy transfer of bacteria from the nose to the middle ear space. This is another reason that children are so prone to middle ear infections. Most children older than 6 years have outgrown this problem and their frequency of ear infections should drop substantially.
Medical Treatment
1) Allergic Treatment and Nasal Decongestion:
Identification and treatment of nasal allergies may also help to reduce the swelling in the lining of the Eustachian tube. Identifying the particular allergen a patient is sensitive to and eliminating it from the environment may reduce the patient's symptoms. Allergy shots may also provide some help, although it may take a long time to notice beneficial effects. Intranasal steroids act to reduce inflammation of the mucosal lining of the nose and may provide some benefit to patients with Eustachian tube dysfunction. In my experience, this helps about 50% of patients with Eustachian tube dysfunction secondary to allergies. A trial of 2 weeks of daily usage is recommended to see if the medication is helpful. Nasal steroids take this long to begin to work. The onset of their effects is gradual, so patients have to use it every day. One does not typically notice an immediate improvement after spraying it in their nose.
Decongestants constrict blood vessels and help open the Eustachian tube by reducing swelling of the lining of the nose. These medications work immediately and can be taken as needed. Oral preparations work for about 4 hours and should not be used around bedtime because they may make it difficult to get to sleep. Nasal spray preparations work quite well and directly decongest the nose; however, because the body rapidly gets used to the medication, they should only be used for up to three days in a row. Antihistamines work to reduce the bodys inflammatory response to allergens. These medications may be helpful for some patients, although in my experience, not as reliably as nasal steroids or decongestants. Antihistamines can be taken as needed.
2) Self-Inflation of the Ears:
It is possible to forcibly blow air through the Eustachian tube into the middle ear by pinching the nose closed and popping the ear. Another way to do this is to blow up balloons. The pressure required to expand a balloon is usually enough to push air up the Eustachian tube. This is a very useful maneuver and may be repeated as often as necessary, whenever a sense of pressure or fullness in the ear develops. This should not be performed when a cold or nasal discharge is present as this may drive infected mucous into the middle ear and cause an ear infection.
Surgical Treatment
The primary goal of surgical treatment is to bypass the Eustachian tube and re-establish ventilation of the middle ear. This will restore hearing, relieve pressure sensation in the ear, and reduce the tendency for middle ear infections.
Myringotomy
A tiny incision can be made in the eardrum and any fluid within the middle ear suctioned out. In adults, the incision often stays open long enough to allow the swelling in the Eustachian tube lining to resolve. After the eardrum heals (usually within 1 to 3 days), the middle ear fluid may re-accumulate if the Eustachian tube lining has not recovered.
Pressure Equalization Tubes
After making an incision in the eardrum and suctioning out any middle ear fluid, a tiny hollow tube made of plastic or metal is inserted into the eardrum. Over time, the tube is pushed out as the eardrum heals. A pressure equalization tube usually provides middle ear ventilation for 6 to 12 months. Often, the Eustachian tube will have recovered by this time and the pressure equalization tubes need not be replaced. However, longer lasting tubes are available for more chronic problems. In adults, the procedure takes about 5 minutes and can be performed in the office using a topical anesthetic. In children, a light general anesthetic is needed.
The major disadvantage of pressure equalization tubes is that water must be kept out of the ear. This requires using earplugs or a cotton ball smothered in petroleum jelly while bathing. Swimming usually requires custom earplugs fit individually to the patients ear. Water that gets into the ear canal can carry bacteria through the tube into the middle ear space and cause an ear infection. This is noted as a purulent drainage (white, green, or yellow pus) from the ear. This type of ear infection can be easily treated with antibiotic eardrops.
The other risk of either a myringotomy or a pressure equalization tube is that the incision may not heal. This may eventually require surgery (tympanoplasty) to patch the hole.
Eustachian Tube Dysfunction Related to Flying
Individuals with Eustachian tube problems may experience difficulty equalizing their middle ear pressure when flying. During airplane travel the ears are subject to large swings in barometric pressure. As you ascend, the cabin air pressure drops and a relative positive pressure builds up in the middle ears. For most people, this pressure easily escapes out through the Eustachian tube. Thus, the pressure of the middle ear equilibrates with that of the cabin air pressure (about 6000 feet above sea level).
Pressure equalization during descent is much more difficult. The cabin air pressure gradually increases during descent. Thus, a relative negative pressure develops in the middle ear that tends to lock the Eustachian tube closed. Yawning, swallowing, chewing gum, or trying to pop ones ears usually will help the Eustachian tube to open at some point, equalizing the middle pressure. Most adults can fly without difficulty unless they have an illness that has temporarily swollen the lining of the Eustachian tube and narrowed its passageway. Some adults have very mild Eustachian tube dysfunction and only have symptoms when flying.
Prevention of Middle Ear Problems with Flying
- Self-Inflation of the Ears
- Swallow frequently during airplane descent
Normally the Eustachian tubes are closed except when you swallow or yawn. Have available some chewing gum, hard candy, or liquid refreshment to assist frequent swallowing while the plane is descending. Do not sleep during the last part of the flight as you may awake with an earache and a Eustachian tube that has already locked closed. - Nasal Decongestion
Decongestant medications help to reduce swelling in the lining of the tube and open its passageway. These medications should be taken so that their peak activity is during the last hour of flight. Generally, oral decongestants should be taken from 2 to 3 hours before the anticipated arrival time while nasal sprays should be used about 1 hour before arrival. - Avoid Flying when you have a cold, the flu, or nasal allergies.
- Pressure Equalization Tubes
Frequent fliers with recurring eustachian tube problems need a more lasting solution. A pressure equalization tube will resolve the symptoms of Eustachian tube dysfunction, although the risks of ear infection and eardrum perforation must be weighed against this benefit