A look back at Stanford Medicine’s efforts to educate, protect and care for patients and members of the public since the World Health Organization declared a global pandemic a year ago today.
March 11, 2021 - By Krista Conger

Rich Brotherton, a research nurse manager at Stanford Medicine, prepares to deliver a dose of Johnson & Johnson's COVID-19 vaccine to clinical trial participant Walter Sobba.
Steve Fisch
As the novel coronavirus spread across the country in the early days of 2020, the faculty and staff of Stanford Medicine worked around the clock to ensure their patients and the public were educated, protected and cared for.
“Even though there were so many unknowns, our people came rolling in the door to help,” recalled Alison Kerr, chief administrative officer of clinical operations for Stanford Health Care. “They were running into the fire, rather than away from it. It was incredibly inspirational.”
As the weeks and then months marched on, plans were upended and a series of grim firsts piled up — first virtual Match Day, first virtual graduations, first day of remote learning, first birthdays away from loved ones.
Now, a year later, we’re commemorating another first: the anniversary of the World Health Organization’s declaration on March 11, 2020, of a global pandemic.
“This past year has been Dickensian,” said Yvonne Maldonado, MD, professor of pediatric infectious diseases and of epidemiology and population health at Stanford. “In many ways, it’s been the best of times and the worst of times. In the face of unprecedented challenges, we were able to pull together to make a real difference in the lives of patients, health care workers and the public. But the pandemic also revealed glaring health care disparities among racial and ethnic groups that must be addressed.”
Throughout the year, the eyes of the nation often turned to Stanford Medicine for answers in a time of uncertainty. Following is a sampling of stories that caught the attention of the public and the media in the subsequent weeks and months.
Testing for infections
It’s hard to stop an invisible enemy, and not every person infected with SARS-CoV-2, the coronavirus that causes COVID-19, has symptoms. Conversely, not every person with a cough, fever, or loss of taste or smell is infected. When clinical virologist Benjamin Pinsky, MD, PhD, associate professor of pathology and of infectious diseases at Stanford, and his team in the clinical virology lab realized in January that it would be critical to have a good, readily available diagnostic test to guide patient care and track the spread of the pandemic, they got to work.

Justin Manalac, a senior clinical laboratory scientist at Stanford Health Care, prepares reagents for testing COVID-19 antibodies.
Steve Fisch
“The Food and Drug Administration had only authorized the test offered through the Centers for Disease Control, which was in very limited supply,” recalled Christina Kong, MD, professor of pathology and medical director of pathology and clinical lab services at Stanford Health Care.
Pinsky and his team worked tirelessly through February to develop one of the first diagnostic tests offered by an academic medical center for identifying people infected with the virus. During that time, Pinsky stopped going home to San Francisco at night and stayed at a hotel near campus to avoid any downtime during a commute that had become complicated.
“People kept calling me, and I’d have to pull off the road to answer their questions and look up the data they needed,” he said in a Stanford Medicine magazine story about the experience. “It wasn’t the safest situation.”
The RT-PCR test they developed was initially used to screen patients at Stanford Medicine who had concerning respiratory symptoms; as capacity ramped up, Pinsky and his team began testing samples from other hospitals in the Bay Area and beyond.
By mid-March, Stanford Medicine was offering drive-through testing for people who had been referred by medical providers at Stanford Health Care’s Express Care, and by April, the lab was offering priority testing to first responders through a new app. The clinical virology lab has to date conducted more than half a million tests.
As Pinsky was developing a test for active COVID-19 cases, pathologist and immunologist Scott Boyd, MD, PhD, was working on another problem: Was it possible to identify people who previously had been infected but recovered? Doing so would be an important step toward understanding the evolution of the pandemic in California and whether a past infection could protect against or decrease the severity of a subsequent infection. It could also help researchers and physicians understand why some infected people became very ill or died, whereas others exhibited few if any symptoms.
In early April, Boyd and his colleagues launched one of the first serology tests to detect the presence in the blood of antibodies to the novel coronavirus, indicating that a person had been infected. “It was a period of intense work,” Boyd recalled, describing 16-hour workdays. “But we were up and running with the test in the clinic by April 7.”
Since then, researchers and clinicians at Stanford have conducted studies showing that self-swabbing is an accurate and safe way to limit medical workers’ exposure to the virus and conserve personal protective equipment. They also demonstrated that pooling samples conserves testing resources when monitoring outbreaks in group settings like schools, nursing homes and prisons, and they launched a surveillance study to identify the presence of new viral variants in the Bay Area.
Detecting symptoms and educating citizens
When the World Health Organization declared the global pandemic a year ago, the public was told to be on the lookout for respiratory symptoms like a dry cough and fever. But soon, people began to report other symptoms. A Stanford Medicine study in April — one of the first to be conducted on coronavirus patients in the United States — detailed a host of gastrointestinal complaints associated with infection, including loss of appetite, nausea, vomiting and diarrhea.

A still image from a video co-produced by Stanford Medicine's Larry Chu for the World Health Organization. In the video, Chu discusses the importance of mask wearing in preventing the spread of the coronavirus.
Larry Chu and Amy Price
The results suggested that people exposed to the coronavirus who are experiencing gastrointestinal symptoms — not just those with respiratory symptoms — should also be tested.
“COVID-19 is probably not just respiratory symptoms like a cough,” the authors said. “A third of the patients we studied had gastrointestinal symptoms. It’s possible we may be missing a significant portion of patients sick with the coronavirus due to our current testing strategies focusing on respiratory symptoms alone.”
Other people began reporting a loss of taste or smell, or both — sometimes the only symptoms they experienced.
Zara Patel, MD, an expert on olfactory disorders, explained why in April.
“A variety of viruses can attack the cranial nerves related to smell or the mucosal tissue that surrounds those nerves,” she said. “Cranial nerves control things in our head and neck — such as the nerves that allow us to speak by using our vocal cords, control our facial motion, hear and smell.”
Not everyone infected required hospitalization, but experts advised patients to monitor their symptoms closely while isolating themselves at home. Stanford internal medicine and Express Care physician Linda Barman, MD, explained to patients what they should do after receiving a positive test result. COVID-19 is typically at its worst around eight to 10 days after symptoms start, so Barman told them to seek medical care if their breathing became more difficult or if they experienced chest pain.
She also warned people about the “shower sign” — that is, when they can’t muster the strength to take a shower.
“That’s happened so many times with people who ended up getting really sick,” she said.
Professor of pediatrics Bonnie Halpern-Felsher, PhD, and her colleagues reported that vaping markedly increases the risk of developing COVID-19 among teens and young adults — populations that had been thought to be relatively unaffected by the virus.
“Teens and young adults need to know that if you use e-cigarettes, you are likely at immediate risk of COVID-19 because you are damaging your lungs,” Halpern-Felsher warned.
Other researchers investigated how best to protect oneself from infection. Larry Chu, MD, and Amy Price, PhD, of Stanford’s Anesthesia Informatics and Media Lab worked with the World Health Organization on guidelines for when and how to wear protective cloth masks, and produced a video detailing the best nonmedical materials for those making their own masks.
Throughout the year, mental health experts offered tips about how to deal with anxiety, get enough sleep(Instagram video) and maintain healthy coping strategies.
“I’ve seen an uptick in stress, a drop of physical activity and dip in social interactions,” said Randall Stafford, MD, PhD, of the Stanford Prevention Research Center, early in the pandemic. “The fallout is likely to exceed the direct harms of COVID-19, but worsening health and well-being also makes us more susceptible to the novel coronavirus and its complications. It’s a good time to take both a break from the news and a few deep, meditative breaths. Don’t let protecting yourself against coronavirus cause your health to take a plunge.”
Understanding the virus
As public concern and interest in the coronavirus grew, virologist Jan Carette, PhD, spoke with Stanford Medicine science writer Bruce Goldman about what a virus is. The two-part series was accompanied by a video that explained how a virus co-opts normal cellular processes to reproduce and spread.
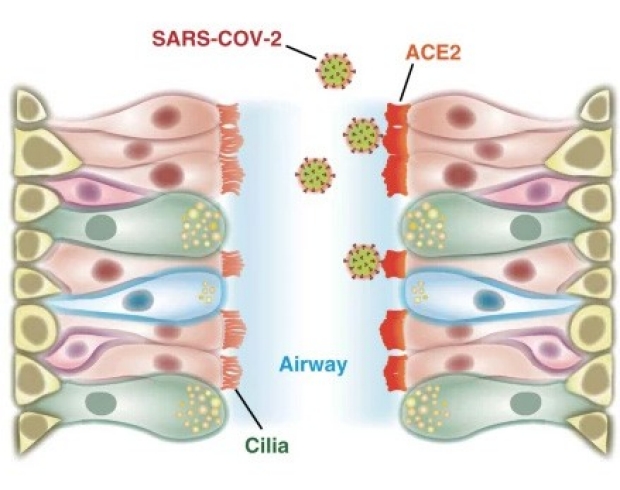
The coronavirus that causes COVID-19 binds to a protein on cells called ACE2, and researchers found high levels of ACE2 in airway cilia.
Tsuguhisa Nakayama
“Outside of a cell, a viral particle is inert,” Carette said. “On its own, it can’t reproduce itself or, for that matter, produce anything at all. It’s the ultimate parasite.”
In the early days of the pandemic, it was thought that a positive test for an unrelated respiratory infection could rule out the possibility that a person was infected with SARS-CoV-2. But by the end of March, researchers at Stanford Medicine published preliminary results indicating that as many as one in five people with COVID-19 symptoms were also infected with other respiratory viruses.
Other researchers doubled-down on efforts to understand exactly how the novel coronavirus affects the immune system, and why some people are more severely affected by it. In August, Bali Pulendran, PhD, professor of pathology and of microbiology and immunology, outlined differences in the immune response between people with mild and severe COVID-19, and in December Scott Boyd and his team reported that the disease severity is affected by the proportion of antibodies that target a critical viral protein — the same protein used in vaccines to train the immune system to reject the virus.
“It remains to be seen whether the immune response to SARS-CoV-2 vaccination is stronger, or persists longer, than that caused by natural infection,” Boyd said. “It’s quite possible it could be better. But there are a lot of questions that still need to be answered.”
Other Stanford studies investigated whether medications given to treat high blood pressure increase the risk of infection (they don’t); identified cells in the upper airways and nasal passages targeted by the virus; and showed that, as of July, few Americans had antibodies to the virus. “This is the largest study to date to confirm that we are nowhere near herd immunity,” Julie Parsonnet, MD, professor of medicine and of epidemiology and population health, said at the time.
Caring for patients
From the beginning of the pandemic, the focus at Stanford Medicine has been on how to care for COVID-19 patients without putting other patients or their health care providers at risk of infection. Early uncertainty about the effectiveness and availability of personal protective equipment, or PPE, necessitated some rapid changes to standard processes and workflows in the emergency department and the intensive care unit. For example, clinicians pivoted to using iPads to establish a personal connection with each patient and allow virtual visits with family members.

Respiratory therapist Dwayne Free confers with nurse Chiara Stetson at Stanford Hospital.
Steve Fisch
“It was nerve-wracking,” said Dwayne Free, one of the frontline respiratory therapists, whose job was to care for these patients at their bedside. “There were so many questions around how the virus was spread. People were scared. Were there going to be enough ventilators? Enough personal protective equipment?”
Routine testing of all patient-facing workers helped establish the effectiveness of the PPE use guidelines and helped health care providers feel secure when Stanford Medicine resumed regular procedures — which had been placed on hold in March of 2020 — in early May of that year. Those COVID-19 patients who were not sick enough to be hospitalized were monitored by the newly established CROWN clinic. “It’s a safe place where we can manage their symptoms and keep them out of the emergency department if it’s not necessary,” said Christopher Lentz, RN, the clinic manager. “We’re hoping this will ease patients’ fears.”
Adjustments were also made to care for patients without COVID-19, including an increase in the use of telemedicine and social distancing as well as patient flow procedures in clinics to ensure that no one needed to delay necessary care. By late summer and early fall, efforts ramped up to prevent a “twindemic” as medical and physician assistant students mobilized to provide flu vaccinations to thousands of people.
Some hospitalized patients were enrolled in the Stanford Medicine arm of a multicenter clinical trial of remdesivir — a potential treatment for COVID-19 that subsequently received emergency use authorization from the FDA.
“To at least have something that we can use as a treatment for this virus is very assuring,” said Aruna Subramanian, MD, a principal investigator of one of the trials. “In the early course of the pandemic, we were all so scared and disheartened by patients going downhill and needing to be on a ventilator for so long. To see that even those people can be turned around is very encouraging.”
In June, Subramanian and infectious disease expert Maldonado launched an ongoing clinical trial of favipiravir— an antiviral drug approved for the treatment of influenza in Japan and of COVID-19 in Russia, China and India — in outpatients with COVID-19.
And in October, Stanford Medicine began enrolling volunteers in a large, phase 3 clinical trial of Johnson & Johnson’s experimental coronavirus vaccine, which received emergency use authorization from the FDA on Feb. 27.
Inequities and vaccine hesitancy
While patient care and research remained a focus at Stanford Medicine, the organization didn’t lose sight of the bigger public health picture. The pandemic revealed vast health disparities among racial and ethnic groups in the United States.

Lloyd Minor and Bill Gates spoke in the fall of 2020 about the impact of the coronavirus pandemic on global health, the race for vaccines and therapeutics, and how to renew the faltering trust many Americans feel in science and medicine.
In November, a Stanford Medicine study found that more than half of the COVID-19 patients who died in U.S. hospitals were Black or Hispanic, and in February 2021, another study showed that an additional 6.8 per 10,000 Black people died of all causes in April of 2020, at the beginning of the pandemic, compared with the average of previous Aprils since 2011. For Hispanics, the rate was 4.3; for Asians, 2.7; and for whites, 1.5.
In some parts of the country, those rates were much higher: “The overall rates of excess mortality and differences by race and ethnicity in New York and New Jersey are absolutely staggering,” said Maria Polyakova, PhD, assistant professor of medicine at Stanford Health Policy and a co-author of the study (subscription required).
“COVID-19 has laid bare a number of injustices and inequities in our own country in health and health care delivery,” said dean Lloyd Minor, MD, in conversation with Bill Gates in October. “The mortality of COVID-19 among communities of color is significantly higher than in white communities. And there’s the sad fact that ZIP code is a more accurate determinant of life expectancy in our country than is genetic code. How as a society do we address these problems that have been in our face for a long time but now are much more difficult to ignore than in the past because of the effects of COVID-19?”
Ensuring equitable vaccine distribution is one way to combat disparity. Yet vaccine hesitancy could become a major barrier to eliminating the threat from the virus. In January 2021, professor of medicine Kevin Schulman, MD, MBA, discussed how to promote vaccine distribution in a politically polarized country.
“Creating a visible symbol of vaccination, like a wearable badge or a digital stamp for social media or Zoom meetings, can help spread awareness and excitement about the vaccine,” Schulman said. “It’s also important to gather and spread success stories on websites and across social media promoting the relief and increased freedom experienced by vaccine recipients.”
As the pandemic recedes, Stanford Medicine leaders have created guidelines to help schools reopen and to advise public officials and business leaders on re-establishing normal operations. The effort is called Recover, Restore and Re-open.
“We see the R3 framework as a collection of resources that community members — whether you’re from academia, industry or government, or you’re an individual — can use to inform and guide how they adapt to the uncertainties wrought by COVID-19,” said Priya Singh, chief strategy officer and senior associate dean for strategy and communications at Stanford Medicine.
And as Stanford Medicine hosts discussions with health care leaders about how the pandemic is changing the practice of medicine, Maldonado, who holds the Taube Professorship of Global Health and Infectious Diseases, reflected on the contributions from across Stanford Medicine during the past year.
“Throughout the pandemic, we’ve had one goal — to keep everyone safe and healthy. Ourselves, our patients, our family members and our community inside and outside of Stanford. Despite moments of stress and sometimes burnout, we knew we were all in this together. As a result, Stanford was able to respond in a way that few other organizations in the world were able to do. It’s been transformative.”
-
 Krista CongerKrista Conger is a senior science writer in the Office of Communications. Email her at kristac@stanford.edu.
Krista CongerKrista Conger is a senior science writer in the Office of Communications. Email her at kristac@stanford.edu.
About Stanford Medicine
Stanford Medicine is an integrated academic health system comprising the Stanford School of Medicine and adult and pediatric health care delivery systems. Together, they harness the full potential of biomedicine through collaborative research, education and clinical care for patients. For more information, please visit med.stanford.edu.

