November 22, 2010 - By Erin Digitale
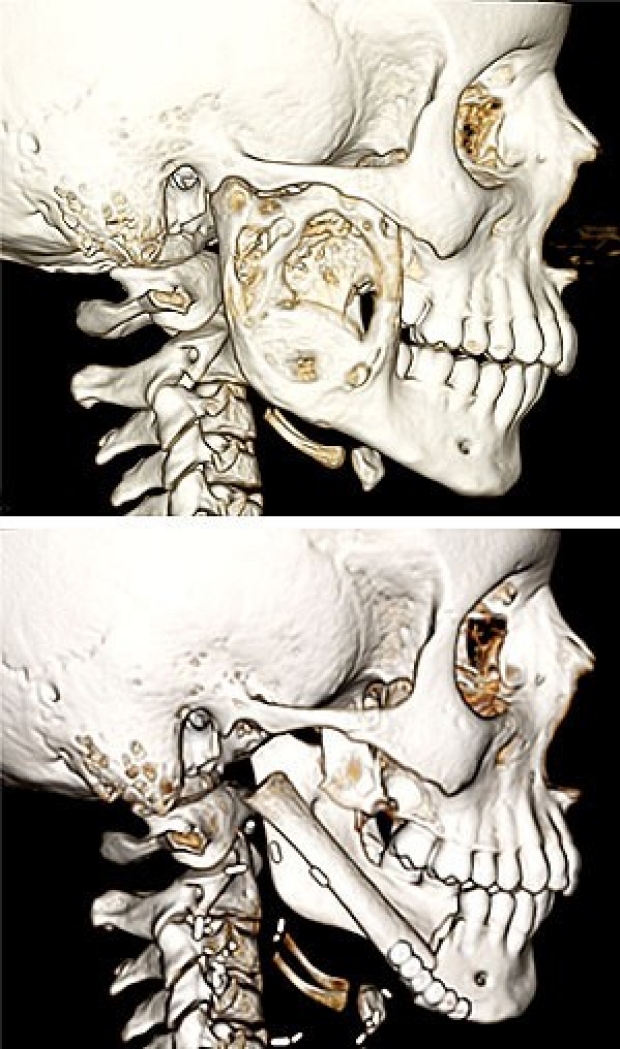
These CT scans show before (top) and after views of an unusual reconstructive surgery to treat a jaw tumor in a 12-year-old boy. Plastic surgeon Rohit Khosla, MD, transplanted a rib with its blood vessels to the patient’s jaw, hoping to give the transplant the fuel it will need to grow in its new location.
Courtesy of Rohit Khosla
Pediatric plastic surgeon Rohit Khosla, MD, had never seen a case like it: The 12-year-old boy’s face ballooned with a rare, aggressive bone tumor. Although it was non-cancerous, the tumor was destroying the patient’s jaw. Khosla knew he would need an innovative approach to save the boy’s ability to chew.
“The situation was pretty complicated,” said Khosla, who practices at Lucile Packard Children’s Hospital. “If he tried to open his mouth, part of the jaw would get stuck. We had to come up with a way to remove all the bone that was involved and reconstruct the mandible.”
To complicate things further, the Bay Area boy, whose family asked that he not be identified for this story, wasn’t finished growing. If his diseased bone was replaced with a static implant, he would eventually outgrow it, leaving his face lopsided.
So Khosla, who is also an assistant professor of plastic and reconstructive surgery at the School of Medicine, decided to try a surgery believed to be the first of its kind in the United States. He would transplant part of a rib to the patient’s face, taking along the rib’s blood vessels to feed the bone and encourage its growth. He hoped the transplanted bone would keep growing, allowing the boy’s face to reach its natural adult shape.
The patient was initially treated by Peter Lorenz, MD, chief of plastic surgery at Packard Children’s. Lorenz diagnosed a chondromyxoid fibroma, a non-malignant bone tumor that usually occurs in the limbs and feet. This type of tissue overgrowth, which looks in CT scans like a patch of bubbly bone, can usually be cured simply by cutting it out.
But in this case, after surgery to excise it, the tumor returned bigger than before. Lorenz and Khosla could soon see that about a third of the patient’s jaw bone, the section extending forward from the temporomandibular joint near his right ear, would have to be entirely removed.
The surgeons decided to try an approach that had been reported in the medical literature only once before. A team in Belgium had described a surgery they nicknamed “the Eve procedure.” They planned to transplant a rib to the face along with its blood vessels and attach this circulation to an artery and vein in the neck.
“Technically, it’s a very demanding procedure,” Khosla said. Even if the microsurgery that hooked up the tiny blood vessels succeeded in the operating room, the vessels could clot off later, necessitating surgical revision.
On the day of the operation, a team of Packard Children’s otolaryngology surgeons removed the diseased jawbone and the tumor. Khosla then cut a 14-cm portion of the patient’s seventh rib from his chest. Ribs are often used in reconstructive surgeries because recovery from loss of one rib is fairly straightforward. And the rib is ideal for replacing one side of the jaw because it consists of a bony end and a cartilage end.
“This allows us to use the cartilage to sculpt a jaw joint, and use the bone to give foundation and structure to replace the bone that was removed,” Khosla said, adding that he also used an envelope of muscle from the rib. This muscle envelope contains the bone-feeding blood vessels and helped fill out the face.
Once he had crafted a replacement jaw joint, Khosla trimmed the rib to fit the gap where the tumor-laden jawbone had been removed. He used about 10 cm of the rib, measuring precisely so that the patient’s upper and lower teeth would line up neatly once the surgery was complete. He fused the rib to the remaining healthy jawbone with surgical plates and screws, then performed the delicate stitch-work needed to attach the blood vessels. He closed the patient’s skin, hiding the scar in the natural skin creases in front of his ear and on his neck.

Rohit Khosla
After the surgery came anxious weeks of waiting. Khosla was relieved that the patient easily cleared the first major hurdle of healing: At discharge from the hospital, his facial circulation to the transplant looked good. The tricky microsurgery had worked – the tiny connections to the rib blood vessels did not clot.
“The other time I felt really good was when he was six to eight weeks out from surgery and was able to chew again,” said Khosla, recalling the boy’s transition from a liquid diet to ordinary food. “I saw that he could eat pretty much whatever he wanted without pain and without restriction in movement of his jaw. It was very reassuring that the reconstructed jaw joint was working well.”
Now, five months after the surgery, the patient continues to thrive. It’s still too soon to know for sure if the transplanted rib is growing, but signs so far look good. And the patient is back to his usual activities: playing soccer, excelling in his seventh-grade math classes and just enjoying being a 12-year-old kid.
-
 Erin DigitaleErin Digitale is the pediatrics science writer for the medical school’s Office of Communication & Public Affairs.
Erin DigitaleErin Digitale is the pediatrics science writer for the medical school’s Office of Communication & Public Affairs.
About Stanford Medicine
Stanford Medicine is an integrated academic health system comprising the Stanford School of Medicine and adult and pediatric health care delivery systems. Together, they harness the full potential of biomedicine through collaborative research, education and clinical care for patients. For more information, please visit med.stanford.edu.

