Scientific News
Double Diffusion Encoding MRI
by Grant Yang, MS(EE), Qiyuan Tian, MS(EE), Christoph Leuze, PhD, Max Wintermark, MD and Jennifer McNab, PhD
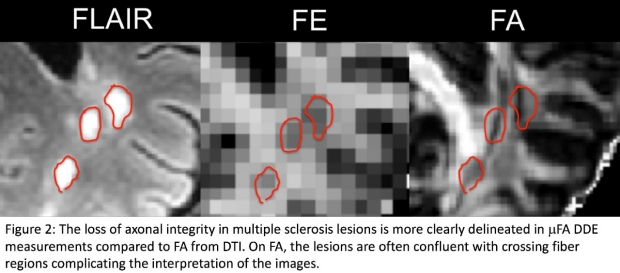
Conventional diffusion imaging is useful for studying white matter microstructure, but detects only the net diffusion anisotropy over an entire voxel. Using net diffusion anisotropy to examine neurodegeneration leads to ambiguity between fiber coherence and axonal integrity, since both a loss of fiber coherence or axonal integrity leads to reduced diffusion anisotropy. Double diffusion encoding (DDE) MRI extends conventional diffusion imaging by encoding diffusion twice before the readout (Figure 1). One application of DDE MRI is to measure microscopic diffusion anisotropy, which reflects the shape of the tissue microstructures independent of their orientation distribution within the voxel. By eliminating the dependence on fiber coherence, microscopic diffusion anisotropy is a more specific measure of axonal integrity. At the Lucas Center, we have implemented a DDE sequence and acquisition scheme, which allows whole brain measurements of microscopic anisotropy in as little as 5 minutes (Figure 2).

Improving MR Thermometry for Tumor Patients Treated with MRgFUS
by Rachelle Bitton, PhD, Pejman Ghanouni, MD, PhD and Kim Butt-Pauly, PhD
A collaborative clinical and research effort between Pejman Ghanouni’s clinical team and Kim Butts Pauly’s lab is offering a new, minimally invasive option to patients with desmoid tumors by treating them with MR guided Focused Ultrasound (MRgFUS). The results of a multi-center study using MRgFUS to treat patients with desmoid tumors have recently been published in European Radiology. The team is working to further improve this treatment option for patients with desmoids and other soft tissue tumors. MR thermometry-derived thermal dose mapping is the primary method used to assess tumor ablation during the procedure. However, it does not account for local accumulation of heat that occurs when treatment times are long. By obtaining a more accurate picture of cumulative thermal dose, physicians can reduce the number of sonications and amount of energy needed for treatment, in turn reducing the risks to the patient.
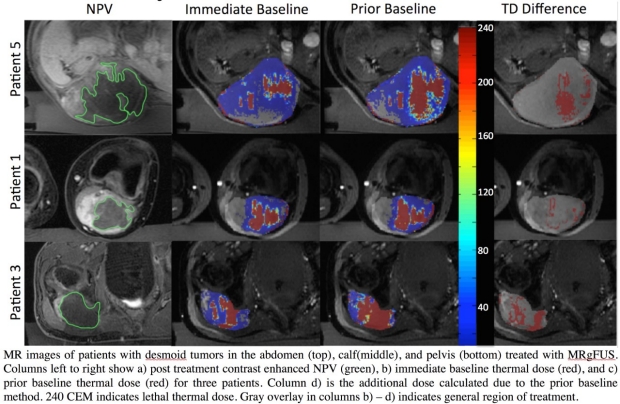
Another recent publication from these researchers describes a long-term thermometry method to account for heat accumulation during treatment. As opposed to the conventional immediate baseline method, the prior baseline approach applied in this study aims to calculate temperature using a baseline image acquired early in a treatment, when ablation induced heat accumulation is minimized, and the assumption of a reference image at body temperature is valid. The prior baseline method is compared against the gold standard of non-perfused volume (NPV) obtained from post-treatment contrast enhanced images.
The retrospective analysis searched previously acquired baseline images for a match in both slice location, using a 2D normalized cross correlation, and in phase variation, using a weighted mean of phase difference images. Thermal dose maps were recalculated using the matched baseline. They showed additional thermal dose that was not accounted for using the conventional (immediate baseline) method. For each patient in the study, the application of the prior baseline method increased the estimated treatment volume and improved the agreement with post treatment NPV (p = 0.023 using a paired two tailed t-test). The team is currently working on implementing a real-time version of this cumulative dose technique for use in patients being treated with MRgFUS.
3D Knee MRI and T2 Mapping
by Bragi Sveinsson, PhD, Akshay Chaudhari, MS, Marcus Alley, PhD and Brian Hargreaves, PhD
Most clinical knee MRI methods are 2D scans that are repeated in different planes, often with different image contrasts, leading to 20-30 minute exams with little or no quantitative information. 3D MRI is used extensively to measure cartilage volume and thickness for research, usually with fat-suppressed spoiled gradient-echo imaging (SPGR), which shows bright cartilage and dark fluid and bone. Faster, quantitative 3D approaches for both morphologic imaging and measurement of relaxation time T2 are now possible using 3D double-echo in steady-state MRI (DESS).
3D DESS is based on gradient echo sequences, and produces two images with different contrast mostly based on T2 differences. The images are simultaneously collected, and can be processed to produce fluid-sensitive images, fluid-nulled images, and T2 relaxation maps. At the Lucas center, such processing can be done automatically during image reconstruction, producing DICOM images for these cases. The customized pulse sequence typically uses water-only excitation to suppress the fat signal, and images with approximately 0.3 x 0.3 x 1.5mm resolution can be acquired in 5 minutes.
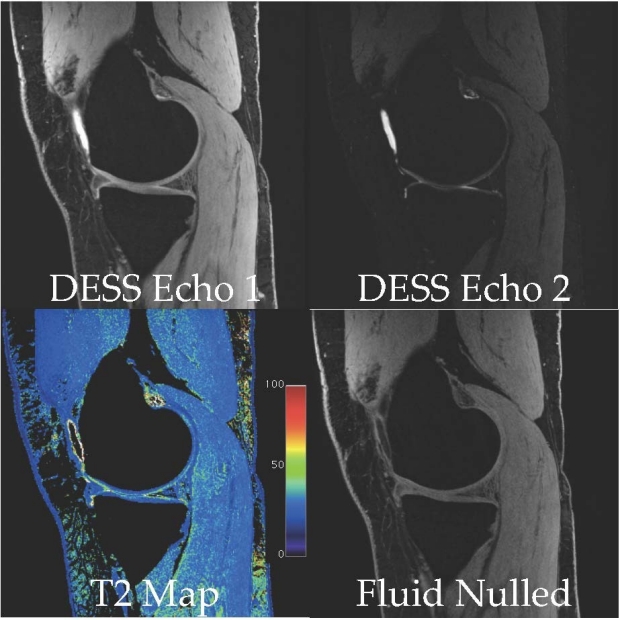
Example images are shown: the source images (DESS 1 and 2), T2 map image, and a fluid-suppressed image (Resolution 0.3 x 0.3 x 1.5mm, 5 min scan time).

Contact-Free Physiological Monitoring
by Julian Maclaren, PhD, Murat Aksoy, PhD, and Roland Bammer, PhD
A user-friendly alternative may exist to the regular pulse oximeter, commonly used for peripheral gating in MRI.
In a study published in the August edition of Magnetic Resonance in Medicine, Lucas Center researchers showed that it is possible to generate a similar signal to that obtained from a conventional pulse oximeter, by monitoring video of a subject’s forehead. Unlike a typical finger-mounted pulse oximeter, this new approach does not require physical contact with the subject. It is therefore potentially more robust in cases where the pulse oximeter can become dislodged from the finger. The technique works by detecting tiny changes in light absorbed by the skin, which occur due to blood volume changes in the subcutaneous tissue during the cardiac cycle.
The scientists, Drs. Maclaren, Aksoy, and Bammer, were inspired by recent work on Eulerian video magnification, and realized that they could apply some of the same principles to their research in the Lucas Center. Because they were already using camera systems in the bore of the MRI scanner for their work on prospective motion correction, they were able to quickly test the concept. They found that although it is not possible to obtain a subject’s oxygen saturation from the signal obtained, it is straightforward to acquire a signal well-suited to triggering or gating the MRI acquisition: a requirement in many scans.
The researchers were also able to detect breathing motion by monitoring microscopic changes in head position using video data. However, this approach is less robust to head motion, so they believe that contact-free detection of the cardiac signal is a more practical application for the technology. A second potential application is patient monitoring. By enhancing the very slight changes in light absorption from the skin, it is possible to generate a visualization of the pulsations relating to the cardiac cycle (see video at right).
The published manuscript described here can be found on the Magnetic Resonance in Medicine website and is also freely available through PubMed.
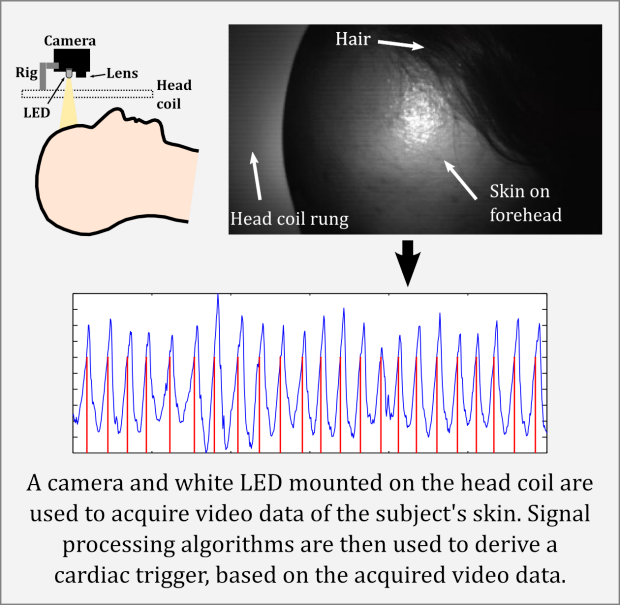
By enhancing the very slight changes in light absorption from the skin, it is possible to generate a visualization of the pulsations relating to the cardiac cycle (see video above).
Simultaneous Multi-Slice (SMS) EPI acquisitions for fMRI
by Gary H. Glover, PhD and Jingyuan Chen, MS(EE)
The (non-definitively named) multiband sequence is available on both 3T2 and 3T3. The sequence was first developed by Atsushi Takahashi, a former postdoc who was working for GE’s Applied Sciences Lab at the time, and it was modified and made practical by Kangrong Zhu, an EE grad student who just graduated (Yay!), then further modified by Bob Dougherty at the CNI, and finally by Jingyuan Chen, another EE grad student and Gary Glover.
The advantage of SMS is that much faster temporal resolution can be obtained because multiple slices are acquired concurrently. A typical TR with SMS factor of 6 (number of simultaneous slices) is 350 msec to acquire 30 slices. This gives some advantage in tSNR because of the larger number of time frames, though the actual advantage is tempered by reduced flip angle due to finite T1 saturation recovery and increased temporal autocorrelation due to sluggish hemodynamic response, and plateau’s at about 30% improvement.
The reconstruction is iterative and currently requires many seconds per image. It is performed with an off-line recon engine with output images (4D .nii format) transferred automatically to the associated dicom computer along with .physio files if acquired. A typical acquisition with 30 slices and 2000 time frames (~11.5 minute scan) will take several hours to reconstruct. It will therefore not be possible to provide motion plots nor examine the images in real time on the scanner. The images that come up on the console as the scan is progressing will be of no value because of the overlapping slices that are only sorted out during reconstruction.
A typical protocol can be found in Adult/Head/gary-episms, which can be copied and modified for your use. Currently Jingyuan Chen is guardian of the sequence.
2016_0613
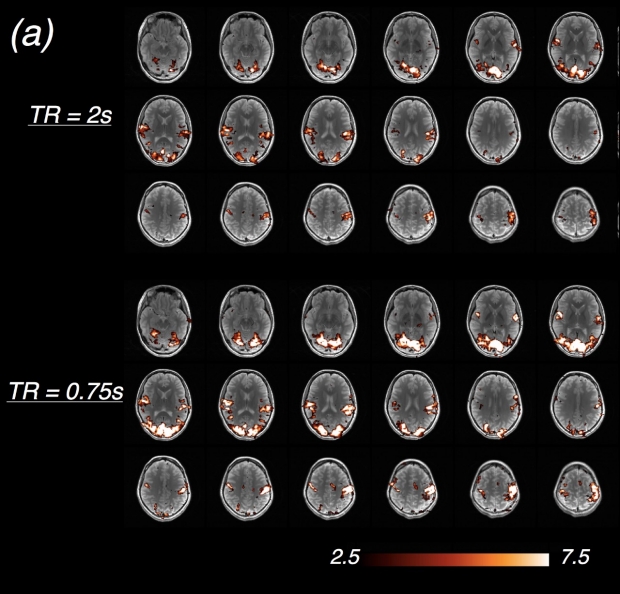
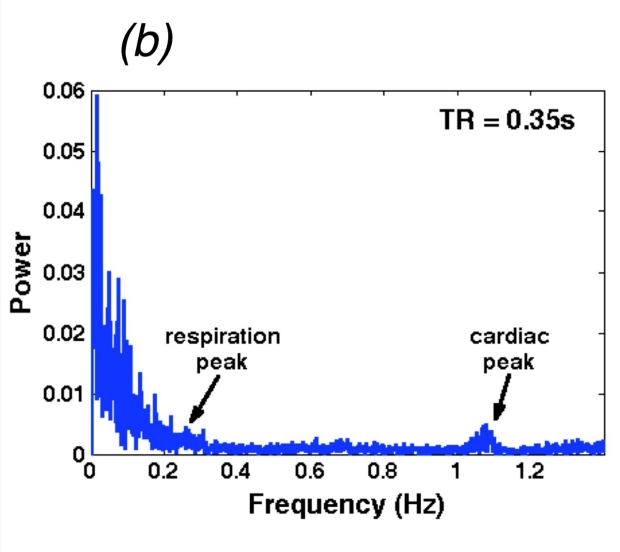
Figures a and b. Compared to spiral in/out, benefits of SMS sequence are primarily two fold: (1) statistical power of a fixed scan duration is enhanced due to increased time frames (a), t-score map of a single subject’s brain activation, visual + auditory block-design task); (2) high-frequency noise, e.g., fluctuations induced by cardiac cycles (b), power spectrum of a single subject’s global signal) won’t alias into low-frequency signal bands, and can be removed through temporal filtering.
Neuroimaging Update
by Michael Moseley, PhD
As a prelude to the Update on Neuroimaging, don't forget the upcoming August 24th 5-630PM second year of the popular “Hammers and Nails” Neuroradiology/RSL discussions. The Hammers and Nails series arose as a way for the RSL MR tools to best suit neuroimaging nails, such as what MR method might best image tumor recurrence from necrosis.
Noteworthy neuroimaging news would include the new MRI “Lucas Mock Scanner” simulator now operational (sans B0 field) outside of the 3T1 in the basement. For more, look here: http://lucasmr.stanford.edu/node/115
Also, in the news from the recent ISMRM in Singapore meeting, several new techniques (“Hammers”) are currently in use or under development looking for that killer app (“Nails”) for which it might best be suited. How do you find these? The new and revised Lucas Center and the RSL webpages (look under the “News” headings) are the best sources. Contact each of the faculty or staff working on a technique, or check back in the Neuro Neighborhood column here for updates.
Perhaps the coolest methods for visualizing brain “motions” are the MRE (“MR Elastography”) and the aMRI (Amplified MRI) methods. Topic of the recent SMRT’s President’s Award, MRE is a measure of brain “stiffness” or compliance. Using low frequency mechanical waves, this might be the best way to image brain compliance or intracranial pressure.
http://med.stanford.edu/rsl/news/eppersonsmrt.html
Also, aMRI is a way of viewing neural compliance using the cardiac output as an internal vibration generator. Once amplified, brain motions can be better visualized.
http://med.stanford.edu/rsl/research/RecentResearch/AmplifiedMRI.html
Where these visualization “hammers” might best be used in still unclear. Have an idea or question? Contact us.
Probably one of the hottest topics in MR today is the incorporation of a new transmit method known as Simultaneous Multi-Slice or “SMS”. Ideal for most 2DFT methods such as GRE-EPI based BOLD (fMRI) and DWI/DTI, SMS (sometimes called Multi-band MRI) can dramatically reduce TR, with EPI images being acquired at as much as 3Hz (TR350ms). Resting state fMRI image series can be acquired well within the cardiac frequencies, which opens an entirely new world of frequency-resolved or “dynamic” resting state fMRI. Since BOLD is in reality largely a perfusion or blood flow phenomenon, dynamic BOLD becomes a fast and versatile noninvasive perfusion measure. Imagine cerebral flow and transit maps, oxygenation studies as well as neural network analyses within a single 2-5 minute series. See what is happening at Lucas with dynamic BOLD; contrast Gary, Greg, or Mike and ask how dynamic BOLD might help your studies.
In more detail, Thomas Christen and Hesam Jahanian from Greg Zaharchuk’s group have studied what can be called spontaneous fluctuations of the MR BOLD signal usually acquired to explore the brain’s functional organization in resting-state BOLD (rsBOLD) fMRI studies. However, a few recent reports have suggested that resting state or dynamic BOLD could also be used for perfusion measurements. The amplitude of BOLD fluctuations could be related to blood volume/flow/oxygenation while delays in the BOLD signal may reflect arterial arrival time.
Winner of the 2014 Young Investigator Award of the ISMRM, Thomas and Hesam compared perfusion maps obtained with rsBOLD (no contrast agent used) to perfusion maps obtained with Dynamic Susceptibility Contrast (using Gadolinium contrast agent) in patients with cerebrovascular diseases.
From a standard echo EPI acquisition, they create maps of rsBOLD Standard deviation by transforming the time series to the frequency domain, and computing the amplitude of signal fluctuations as the squared root of the average of the power spectral density for each voxel. rsBOLD time lag maps are created by manually delineating a region of interest over the superior sagittal sinus vein. A cross correlation analysis is performed between this ‘seed’ signal and all other brain voxels. The analysis is also performed with the reference signal shifted from +/-5TR to account for possible time delays. The rsBOLD lag maps are eventually derived by taking the maximum of the correlation coefficient over the time lag.
The figure below shows why there is so much excitement around dynamic resting state fMRI (Figure courtesy of Thomas Christen, PhD).
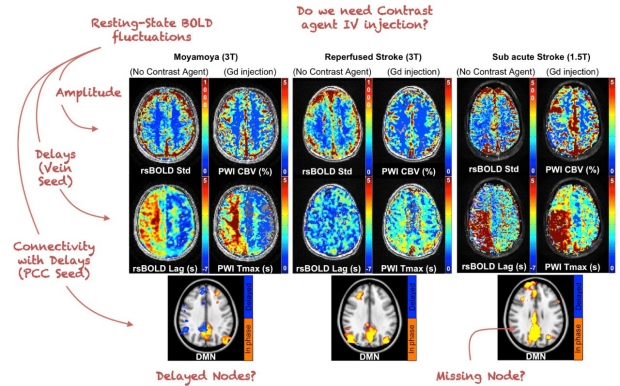
Figure courtesy of Thomas Christen, PhD
One of the first immediate applications of a new and novel method like dynamic BOLD was to study perfusion abnormalities in MoyaMoya patients. Resting state fMRI has been increasingly used to probe alterations of functional organization in neurological or psychiatric diseases. In rsBOLD fMRI, functional networks are assessed using the temporal correlation between spontaneous BOLD signal fluctuations of spatially remote areas of the brain. They have created a pipeline to acquire resting-state fMRI data and create automatically maps of the 10 most common resting-state networks.
In neurological diseases where there are significant delays in different areas of the brain, standard rsBOLD fMRI analysis, both seed-based and using independent component analysis (ICA), may lead to erroneous identification of functional connectivity networks. In an effort to investigate the effects of these transit delays on rsBOLD fMRI, dynamic BOLD was used to study networks (see default mode network (DMN) above) in Moyamoya and stroke patients and compare it with normal healthy volunteers. We also proposed for the first time a functional connectivity analysis method that accounts for transit delay.
We expect that with SMS and rapid functional MR methods in use at Lucas will be rapidly available for a host of other applications in acute stroke, stroke rehabilitation, diseases of the aging, and learning. Have an idea where you might find dynamic BOLD useful – let us know!!
Lucas RSL is not just neuroimaging with MR either. Seek us out for the latest in novel X-ray/CT (Kerstin Mueller), functional neuroimaging (Roland, Gary, Jennifer, Mike M, Brian R, Max, and Greg and Mike Z), Ultrahigh-field 7T MR (Brian R and Jennifer), ultrasound (Jeremy), MRgFUS (Kim and Pejman), Metabolic MR (Dan), and Body MSK (Bob, Brian H, Garry, Bruce, and Shreyas). Think “Hammers and Nails” when you think of the vast and varied imaging toolbox in the Lucas Room of Requirement.