Understanding ILD
Interstitial Lung Disease refers to a large group of lung disorders that cause inflammation or scarring in the lung tissue.
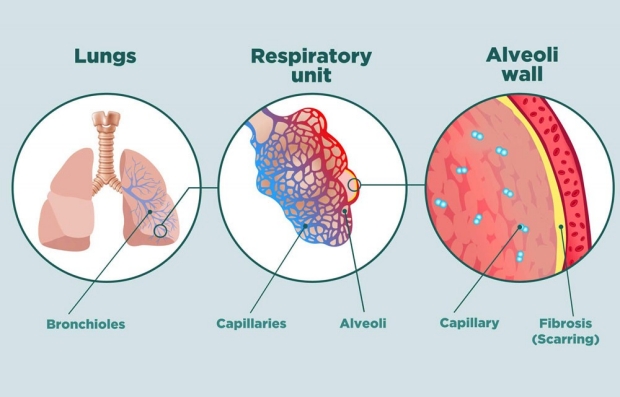
The term “interstitial” refers to the area that surrounds the airsacs (alveoli) of the lung. This interstitial space is where the oxygen that you breathe in moves across the wall of the alveoli and into the small blood vessels (capillaries). Once the oxygen crosses this alveolar-capillary membrane into the blood stream, it is delivered to your brain, muscles, kidneys, and other vital organs. The interstitial space around the alveoli can become inflamed, thickened or scarred because of a variety of insults or reactions in the lungs.
Interstitial Lung Disease (ILD) refers to a group of problems in the lung that affects the “interstitium”. The interstitium refers to the tissue area in and around the wall of the airsacs (alveoli) of the lung area where oxygen moves from the alveoli into the capillary network (small blood vessels) that covers the lung like a thin sheet of blood. Once the oxygen crosses the interstitial space it enters the bloodstream and is delivered to the vital organs of your body. ILDs cause this interstitial space to become inflamed or scarred making it more difficult for oxygen to get into the bloodstream. This inflammation and scarring also makes the lung a bit stiffer which can increase the 'work' of breathing and make you feel more breathless than normal, especially with exertion such as walking up stairs. The changes in the lung tissue can also cause a dry, hacky cough for some patients.

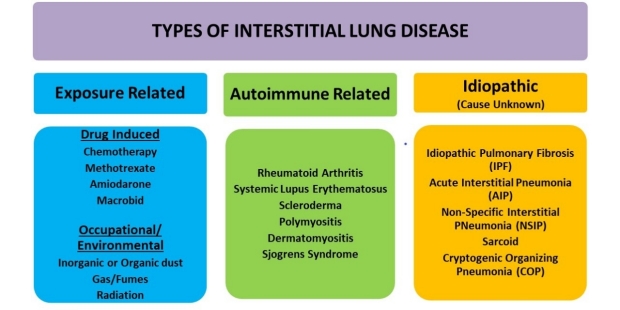
There are many causes of ILDs and they can be categorized as pictured above into three broad, main groups:
- Exposure-Related
- Autoimmune-Related
- Idiopathic, or with no known cause.
These three groups of ILDs have slightly different presentations, and different findings on the CT scans, lung tissue biopsy (if done), and bloodwork results. Each group also has different treatment choices which is why getting a correct diagnosis is extremely important.
Exposure-Related (Hypersensitivity Pneumonitis or 'HP'):
- Inhalation-related:
- There are more than 300 causes of inhalational exposure-related ILDs.
- These exposures can be experienced in the workplace, at home, while doing hobbies, or during travel.
- It is estimated that over 50% of the time the specific exposure is never identified. An "HP Panel" can be ordered to identify whether or not you have been exposed to certain "antigens", such as birds. However, even if this testing documents that you have developed antibodies for a particular antigen, it does not necessarily mean that is the definite cause of your HP.
- When being evaluated for exposure-related ILDs, your physician may ask you to complete an “Exposure History” questionnaire and will also ask you many questions about your history to see if there may be risk factors that we can identify. Some of the more common exposures are mold, birds in or around the home, bedroom, or backyard, farming/agricultural work, indoor hot tubs, standing water, down feathers, and cleaning chemicals.
- Historically, coal miners (pneumoconiosis) and exposure to asbestos (asbestosis) were significant problems, but these exposures have lessened due to the use of protective respiratory equipment.
- Having any of the above exposures does not necessarily mean that you will develop a lung problem. For reasons that are not completely understood, some persons are at increased risk of having a lung reaction to exposures than others.
- If you undergo a lung biopsy, the pathologist can confirm a diagnsosi of Hypersensitivity Pneumonitis by findings in the lung tissue.
- There are more than 300 causes of inhalational exposure-related ILDs.
- Medication-related:
- While ILDs due to a medication are less common than inhalation-related ILDs, they do occur.
- Just like the inhaled exposures, it is important for your physician to obtain a detailed medication history during your ILD evaluation, especially as it relates to timing of the medication with changes in your lung symptoms.
- Some of the medications that can cause an inflammatory reaction in the lung include amiodarone, methotrexate, some chemotherapy agents used to treat cancers, and nitrofurantoin (sulfa drugs).
- Radiation-Exposure related: Some people have had radiation exposure in their chest area, such as with breast cancer treatment. Radiation-induced lung scarring is another cause of ILD.
Autoimmune-Related ILDs (Nonspecific Interstitial Pneumonitis – NSIP):
- Autoimmune refers to your body having some type of inflammatory reaction that results in the development of antibodies that are detected with a blood test. Some types of autoimmune disease can cause inflammation and scarring in the lung. The pattern on the CT scan most often seen with autoimmune-related ILDs is non-specific interstitial pneumonitis; this description can also be used when describing a lung tissue biopsy sample by the pathologist.
- Many autoimmune diseases are associated with physical signs such as rashes, changes in the skin and hands, inflammation of joints, muscle soreness or weakness, and dry eyes and mouth.
- Autoimmune–related ILDs tend to occur more often in women and in persons under the age of 65.
- Examples of autoimmune diseases are rheumatoid arthritis, dermatomyositis, polymyositis, Sjogrens Syndrome, Scleroderma, and vasculitis.
- A diagnosis of an autoimmune disease is made by blood tests known as 'serology' that detect and measure the level of certain antibodies in the blood.
- In some patients, a diagnosis of an autoimmune disease is made first, and then a few years later the autoimmune lung disease manifests itself as an ILD. In other patients, the ILD lung problem may occur first and then a few years later the autoimmune disease may develop with changes in the skin, joints, and positive serology.
Idiopathic ILDs (no known cause):
- Idiopathic Pulmonary Fibrosis (IPF) is the most common ILD that has no known cause.
- IPF is also referred to as Usual Interstitial Pneumonia or UIP. UIP describes the particular pattern seen on the CT scan, and can also be used by the pathologist to describe the lung tissue findings if a lung biopsy was done.
- The diagnosis of UIP is made by determining if the pattern on the CT scan is either definitive or possible for UIP, and by eliminating other causes of ILD such as autoimmune disease or an exposure.
- There is research identifying specific ‘biomarkers’ of IPF that occasionally (<20%) occur in families (familial IPF), but the cause of IPF is poorly understood. It more commonly occurs in men, ex-smokers, and usually occurs between the ages of 60 and 80. There are now some blood tests available to check for genetic causes of IPF and ILDs.
- In 2014 two new anti-fibrotic drugs were approved for the treatment of IPF Ofev (nintedanib) and Esbriet (pirfenidone). Both of these medications slow the progression of IPF, but do not stop the process or remove the existing scar tissue.
- Other Idiopathic ILDs: Other ILDs with no known cause include some cases of non-specific interstitial pneumonitis (NSIP), cryptogenic organizing pneumonia (COP), and Sarcoidosis. In some cases the cause of the ILD may be unknown or 'indeterminate' in which case a patient might undergo a surgical lung biopsy, or a transbronchial biopsy with bronchoalveolar lavage in order to get additional information to make a diagnosis.
Shortness of Breath (Dyspnea):
Most patients seek a physician evaluation after noticing shortness of breath (dyspnea) usually with exertion, such as walking up stairs or a hill. The start of breathlessness can be very gradual and many patients initially think they are either just ‘out of shape’ or ‘getting older’ but eventually seek an evaluation. In some cases, breathlessness can occur more rapidly if, for example, you experienced a significant exposure. A diagnosis of ILD can also follow an episode of bronchitis or flu that does not easily go away with treatment. At some point, your physician may order a chest x-ray or a CT scan and an interstitial abnormality is noticed. The treatment of shortness of breath related to ILDs consists of multiple approaches, including treating the underlying lung problem with medications if appropriate, using oxygen if indicated, getting education re: breathing techniques, participating in an exercise program such as Pulmonary Rehabilitation, and getting emotional support through ILD support groups. Working with a Palliative Care physician also provides strategies to cope with the many symptoms that patients and families experience with a new diagnosis or a chronic health problem.
Cough:
Almost 80% of patients with IPF notice a dry bothersome cough. It is often triggered by activity, talking, laughing, singing, or eating. Many patients with other ILDs such as the exposure-related ones (HP or hypersensitivity pneumonitis) may also notice a cough. It is typically dry or ‘non-productive’ but some patients do have sticky mucus that they notice is particularly bothersome in the mornings. A typical evaluation for an ongoing cough will include ruling out three common causes of cough: asthma, gastroesophageal reflux disease (GERD), and upper airway cough syndrome (UACS, commonly referred to as post-nasal drip). Even when those three problems are treated or eliminated, the dry cough from ILD can persist and be difficult to treat.
Depression and Anxiety:
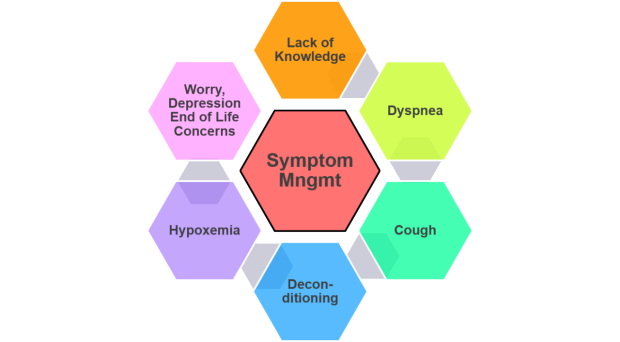
It is not unusual for patients with a new diagnosis of any disease to experience difficulty in coping with the uncertainty of what lies ahead, the changes in lifestyle due to various symptoms or medication side effects, and a lack of understanding about the disease itself. Friends and family members are also affected. The approach to managing symptoms for patients with ILD is multifaceted and takes a number of interventions including gaining support and education, learning about pulmonary rehabilitation, understanding medications, and using oxygen appropriately if needed. Feeling short of breath can understandably be very anxiety-provoking both for you as the patient and for your caregivers. The diagram below illustrates how addressing exercise, education, emotional support, and oxygenation can improve quality of life for patients with ILD.
How would I know if I have ILD?
- Symptoms: Most patients may find out that they have some type of ILD because of noticing shortness of breath and/or cough:
- Many patients find that they are more short of breath with activities such as stair climbing or walking up an incline, but may feel that it is simply from being 'out of shape' or 'getting old'.
- Some patients may notice a dry, hacking, nagging cough that never goes away despite trying various medications.This might lead to obtaining a chest x-ray and at that time the radiologist may note 'interstitial markings' on the film.
- Eventually most patients may seek their physician's help when these symptoms get worse and an x-ray or CT scan of the chest is ordered.
- X-Ray or CT scan of the chest:
- The definitive test for ILD is a high resolution computed tomography scan (HRCT scan) of the lungs. This type of x-ray allows the radiologist and pulmonologist to see the changes in the tissue pattern in the lung. A regular chest x-ray might also show interstitial abnormalities but it is not sensitive enough to make an ILD diagnosis.
- Most patients have a CT scan done because of lung symptoms that they are experiencing. Other patients may not be experiencing any respiratory symptoms, but have a chest x-ray or CT scan for another non-respiratory reason (upcoming surgery for example), and interstitial markings are found on the test.
What would happen next in order to make a diagnosis of ILD?
- You would be referred to a lung specialist to further evaluate the abnormal findings seen on your CT scan.
- Additional testing would be ordered (see next section for list of testing) including breathing tests and blood work.
- You may be referred to a specialized ILD Clinic.
Radiology evaluations:
- A Computed Tomography (CT) scan of the chest is the most sensitive diagnostic tool for ILD. The best assessment is with a high resolution CT scan (HRCT) which provides thin slices (1-2 mm thick) of the lungs in order to closely evaluate the lung tissue changes. The initial HRCT scan may also include views done while lying on your stomach (prone), and lying on your back during full inspiration and during full expiration. Once a patient is found to have possible findings of ILD on a chest CT scan, the next step is to confirm the type of ILD.
- Chest X-Rays may show ILD but are not diagnostic.
Breathing tests:
Pulmonary Function Studies (PFTs) are used to evaluate the severity of the lung problem. PFTs evaluate the ability of the lung to:
- move air in and out of the lungs (spirometry- Forced Vital Capacity (FVC), Forced Expiratory Volume in 1 second (FEV1)
- take in a large breath or measure how ‘restricted’ or limited the total lung volumes are (lung volumes or plethysmography)
- transfer oxygen from the lung air sacs into the bloodstream (diffusion capacity)
PFTs repeated over time are also used to determine how you respond to medication treatment, and if your ILD is stable, improving, or worsening over time. PFTs are typically measured about every 3-6 months depending on your individual case.
Exercise and Oxygen Studies:
- Six Minute Walk (6MW) Test is a standardized test used to evaluate the distance that you are able to walk in 6 minutes. A 6MW can also show how your oxygen levels are maintained during activity or exercise, and how breathless you are with exercise. The oxygen saturation is measured using a pulse oximeter on your finger or forehead while you walk quickly to cover as much distance as possible in six minutes. This is an important assessment because 6MW distance has been correlated with overall prognosis. For some patients, performing this measurement at regular intervals (every 3-6 months) provides clinicians important information to assess disease progression or stability, and also responses to drug therapy.
- Oxygen Titration Testing: If you were found to have a low oxygen level during walking as measured by a pulse oximeter on your finger or forehead, we will walk you again in order to determine exactly how much oxygen (liter flow or number setting) that you need with exertion.
- Cardio-Pulmonary Exercise Testing (CPET): In some individuals there may be both a heart and a lung problem and it can be difficult to know if your shortness of breath is from a lung problem or heart problem, or both. A CPET is a more thorough exercise study that uses extensive monitoring to measure oxygen levels, metabolism, electrocardiogram monitoring, and exhaled gas measurements. Results can identify if a cardiac problem is contributing to or causing your symptoms.
Lung Tissue Sampling: If the decision is made that a lung tissue sample (lung biopsy) is needed in order to make a diagnosis, there are a few different options:
- Transbronchial Biopsy (TBBx) with Bronchoalveolar Lavage (BAL) can be done to obtain a very small piece of lung tissue and also a sample of a ‘washing’ of sterile water in and out of the lungs. It is performed as an outpatient procedure. You are admitted to a short stay unit, undergo sedation, and have a thin tube or endoscope passed through your mouth into your trachea down into your airway. A small forceps is used to get a couple of tiny pieces of lung tissue for pathology analysis. This type of lung biopsy might help us know what type of ILD you may or may not have, but is typically not definitive due to the very small size of the tissue sample. The lavage fluid is also tested for types of cells and the presence of any infection and may help us determine one type of ILD vs another; the fluid testing can also eliminate some types of ILD.
- Cryobiopsy is a more recent procedure available at Stanford and some other centers that is done similarly to a TBBx but allows for obtaining a larger piece of lung tissue. This is done by passing a specialized endoscope into your lungs that has a tip that freezes a section of lung tissue and then withdraws it for analysis.
- Video-Assisted Thoracoscopic Surgical lung biopsy or ‘VATS’ surgery is performed when the physicians are unable to determine your diagnosis or the cause of your ILD and have determined that you would be a candidate for this procedure. This is a surgical procedure that involves placing scopes into about three different small incisions on the side of your chest. One of them uses forceps to obtain a sample of lung tissue, often from 2 or 3 different areas of you lung on one side. You are admitted to the hospital for a few days, undergo general anesthesia, and will have a tube temporarily placed into the side of your chest during the surgery to help the lung re-expand. This tube will be removed after surgery once the lung is re-expanded.
Blood Tests: There are different types of blood tests that may be ordered to assist in making an accurate diagnosis
Serology: These are blood tests that look for antibodies (proteins made by your immune system) in your blood to determine if you have a type of autoimmune disease (lupus, slceroderma, Sjögren's sydrome, polymyositis/ dermatomyositis, mixed connective tissue disease). Examples of these blood tests include:
- Rheumatoid Factor: rheumatoid arthritis
- ESR: estimated sedimentation rate
- CRP: C-reactive protein reflecting a response to inflammation
- ANA: Antinuclear Antibodies
- anti-dsDNA: anti-double stranded DNA
- anti-SSA (Ro) and anti-SSB (La): anti Smith antigens
- Anti-JO-1
- ANCA: antineutrophil cytoplasmic antibodies
- anti-Scl 70: scleroderma
Genetic Testing: In some patients, there is a strong family history of pulmonary fibrosis, defined as at least two or more family members being diagnosed with pulmonary fibrosis. In some cases, we may recommend genetic testing including:
- Telomere Length Measurements:
- Interstitial Lung Disease Panel, Prevention Genetics:
Shortened telomeres have been associated with the development of familial pulmonary fibrosis- an inheritable form of pulmonary fibrosis that can be passed down from one family member to another. This test is usually covered by insurance, but patients will need to call their insurance prior in order to confirm. The decision to perform this test will be made after a comprehensive review of the patient’s history.
This test includes genetic screening for a large group of more rare pulmonary diseases, including Familial Pulmonary Fibrosis, Neurofibromatosis, Tuberous Sclerosis, Birt-Hogg Dube Syndrome, Cystic Fibrosis, Hermansky-Pudlak syndrome, and others.
Consultation with Other Specialists: Because ILDs often involve other medical issues we frequently refer patients for evaluation by other medical specialists.
- Rheumatology/Immunology: To evaluate for the possibility of autoimmune disease
- Gastroenterology: To evaluate for the presence of reflux that could be worseining cough or other lung symptoms
- Cardiology: To evaluate if a cardiac problem is causing or adding to breathlessness or other problems
- Genetics Counselor: To discuss the meaning of any genetic testing related to ILD and how it may affect treatment, family, children, etc…
Pharmacologic (drug)Treatment:
- General:
- Several different medications have been used for the treatment of ILDs. Only your pulmonary specialist can determine whether you need to take medication to treat your particular ILD. The following is a list of medications sometimes used by doctors to treat ILD. It is extremely important that if you are taking any of these medications, you should be closely monitored by your physician. This includes obtaining frequent bloodwork monitoring while you take these medications, especially in the beginning.
- Immunosuppressive Medications: Drugs that suppress inflammation in the lung:
- Corticosteroids (prednisone): Prednisone is used to suppress the immune system and to decrease the inflammation in the lung, sometimes described as ‘ground glass opacities’ or white fluffy markings that are seen on the CT scan. Steroids mimic the action of cortisol that is produced by the adrenal glands. Prednisone has many side effects which require careful monitoring, particularly elevation of blood sugar levels, effects on vision, and bone-thinning. It may be used when there are signs of inflammation on your CT scan, during an acute exacerbation, or, in some cases, at low dose to help control cough. When prescribed it is very important to confirm the dose and the schedule for any dose lowering, or ‘tapering’ of the medication. Prednisone should not be abruptly stopped if you have been on it for more than a few days.
- Azathioprine (Imuran®): Imuran® is used to suppress the immune system and is commonly used to treat autoimmune diseases such as rheumatoid arthritis. It can also be used either in addition to prednisone, or instead of prednisone to suppress inflammation in the lung in patients with hypersensitivity pneumonitis. It is also used to help prevent the body from rejecting organs following transplantation. It has not been found to be effective in the treatment of IPF based on national clinical treatment trials.
- Mycophenolate mofetil (Cellcept®, Myfortic®): Mycophenolate modulates the immune system and has been used alone or in combination with corticosteroids for several autoimmune disorders, and also with some patients with hypersensitivity pneumonitis when used with or following prednisone.
- Cyclophosphamide (Cytoxan®): Cytoxan® is a chemotherapy agent that can suppress inflammation and has been used to treat certain forms of ILD. It is traditionally taken orally but may also be administered intravenously.
- Bactrim: Bactrim is a combination of sulfamethoxazole and trimethoprim. These are both antibiotics that treat certain infections. Bactrim is sometimes prescribed to patients with ILD who are receiving immunosuppressive drugs such as prednisone or Cellcept (mycophenolate mofetil). These patients are at risk of developing pneumocystis pneumonia because their immunosuppressive treatment may allow these bacteria to grow.
- Anti-Fibrotic (anti-scarring) Agents:
- Nintedanib (Ofev®): Nintedanib is an anti-fibrotic drug that is FDA- approved in the United States to treat IPF and also Scleroderma-related lung fibrosis. It is classified as a Tyrosine Kinase Inhibitor whose action is to block three different substances that are involved in the formation of scar tissue. In clinical trials, nintedanib was shown to slow the decline in lung function in mild-to-moderate IPF. It is a pill taken orally at either 100 or 150 mg twice daily. When you are taking Ofev® it is important to have regular blood tests and to be followed closely by your lung physician, especially liver function tests. The most common side effect of Ofev® is diarrhea, nausea, abdominal pain, vomiting, decreased appetite, and increased liver enzymes. View the FDA drug insert.
- Pirfenidone (Esbriet®, Pirfenex®, Pirespa®): Pirfenidone is an anti-fibrotic and anti-inflammatory drug approved to treat IPF. Its mechanism of action is unclear but it slows the scarring process in the lung. Esbriet® was shown to slow progression of mild-to-moderate IPF as measured by breathing tests (PFTs)- specifically by the Forced Vital Capacity (FVC) which is the amount of air you can forcefully exhale. Esbriet® is taken three times daily as either two to three 267 mg capsule three times/day, or as one 800 mg capsule three times/day. The most common side effects are fatigue, headache, dizziness, skin rash and photosensitivity (sun related rash), nausea, diarrhea, abdominal pain, loss of appetite, and heartburn. View the FDA drug insert.
- Nintedanib (Ofev®): Nintedanib is an anti-fibrotic drug that is FDA- approved in the United States to treat IPF and also Scleroderma-related lung fibrosis. It is classified as a Tyrosine Kinase Inhibitor whose action is to block three different substances that are involved in the formation of scar tissue. In clinical trials, nintedanib was shown to slow the decline in lung function in mild-to-moderate IPF. It is a pill taken orally at either 100 or 150 mg twice daily. When you are taking Ofev® it is important to have regular blood tests and to be followed closely by your lung physician, especially liver function tests. The most common side effect of Ofev® is diarrhea, nausea, abdominal pain, vomiting, decreased appetite, and increased liver enzymes. View the FDA drug insert.
- Anti Reflux Medications:
- Proton pump inhibitors (Prilosec OTC®, Nexium®, others): These drugs help block the formation of acid in the stomach, and are commonly used to prevent and treat gastrointestinal problems, including peptic ulcer disease and gastroesophageal reflux disease (GERD).
- H2 Blockers (Zantac®, Pepcid®) can also be used, especially at nite, to decrease symptoms of GERD or heartburn.
- Common drug treatment specific to different ILDs: Drug treatment is very individualized and can vary person to person. Below is a very general list of medications often used for each type of ILD, but these can vary per individual case.
- Idiopathic Pulmonary Fibrosis (IPF): Ofev® or Esbriet®
- Hypersensitivity Pneumonitis (HP): Steroids (prednisone), sometime initially with or without Imuran®, Cellcept® and then steroids may be gradually tapered so that a single drug such as Imuran® or Cellcept® is used as needed
- Autoimmune Lung Disease: Steroids if needed, Cellcept®, Cytoxan, Methotrexate, Rituximab
- Unclassifiable Interstitial Lung Disease: Prednisone, with possible combinations as above.
- Idiopathic Pulmonary Fibrosis (IPF): Ofev® or Esbriet®
- Several different medications have been used for the treatment of ILDs. Only your pulmonary specialist can determine whether you need to take medication to treat your particular ILD. The following is a list of medications sometimes used by doctors to treat ILD. It is extremely important that if you are taking any of these medications, you should be closely monitored by your physician. This includes obtaining frequent bloodwork monitoring while you take these medications, especially in the beginning.

Courtesy of Cardiac & Pulmonary Wellness, Pulmonary Rehabilitation Program, El Camino Hospital, Mountain View, CA
Benefits of Pulmonary Rehabilitation
Pulmonary Rehabilitation (PR) is a structured exercise and education program for people with chronic lung diseases, including ILDs, with the goal of maximizing a patient’s ability to maintain activity, decrease breathlessness and fatigue, and improve quality of life. Typically, pulmonary rehabilitation will include exercise training (aerobic, strengthening, flexibility); breathing exercises; anxiety, stress, and emotional management strategies; nutritional counseling; disease education; medication education, and other components. This treatment has become an important part of the standard of care for people with chronic lung diseases, and recent studies indicate that pulmonary rehabilitation improves exercise capacity, decreases symptoms, and improves quality of life. Pulmonary Rehabilitation programs offer a variety of services and can be done in the hospital, or as an outpatient in a hospital or community-based program, or sometimes in the home either in person or ‘virtually’ by video/telemedicine. Outpatient programs are typically 8-12 weeks in length for about 2-3 hrs. per day, two or three days per week. Exercise is very individualized and participants are sent home with a home exercise prescription to do on the days they do not attend the PR program.
After completing the 8-12 week program, many PR facilities offer a "Maintenance" program which is just the exercise component about 2-3 times/week for about an hour. Medicare and other insurers typically cover the initial program, but most do not cover the maintenance portion.
One of the key successes of PR programs is breaking the inactivity/shortness of breath cycle that is common for persons with lung problems. Gradually over time, many people tend to avoid those activities that make them breathless and eventually become more sedentary and quite deconditioned leading to the loss of muscle strength. This can cause more breathlessness with activities. PR helps get you moving again and teaches breathing and pacing techniques to help decrease and cope with the breathlessness during exertion.

Coping with a new diagnosis, new medications, and the symptoms of interstitial lung disease can be challenging. Having interactions with other ILD patients and family members, and also receiving accurate information, can be extremely helpful. In addition to in-person ILD support groups, there are also online and phone-in ILD support groups.

Oxygen FAQs
Q. Why do some patients with ILD need to use supplemental oxygen?
A. The purpose of the lung is to transfer the oxygen that we inhale into the bloodstream, and also to remove (exhale) carbon dioxide out of the bloodstream and lung. The transfer of these gases occurs right at the interstitial space, the ‘wall’ between the airsac (alveoli) and the blood vessel (capillary). In ILDs, inflammation and/or scar tissue can build up around this area between the airsac and the blood vessel (alveolar-capillary membrane), and this area becomes thickened. These changes in the interstitium slow down the movement of oxygen from the air sacs into the bloodstream, particularly during periods of physical activity. When oxygen levels drop in the blood, many people become breathless and this limits their daily activities. Normal oxygen levels are 96-98% measured by a pulse oximeter on your fingertip or forehead. Typically, oxygen levels should be kept above 88-90% as measured by a pulse oximeter.
Q. How do I know if I need oxygen?
A. Oxygen is not prescribed by how you feel but instead is prescribed by testing your oxygen levels under different conditions of rest, exertion, and sometimes during sleep. If the results of testing show that your oxygen levels are below 89%, you may be prescribed supplemental oxygen. Your oxygen levels can be tested with a Six Minute Walk test, or Exercise Oximetry:
- A Six Minute Walk Test: During this formal test procedure, the therapist will give you instructions to walk in order to cover as much distance as possible in six minutes. They will check your oxygen levels before you start, and either during walking or right when you stop. If your oxygen levels fall below 89%, you meet national (Medicare) criteria to use oxygen with activity.
- Oxygen Titration Testing: This is a more informal test that not only checks to see if your oxygen levels drop during walking, but also to determine how much oxygen (what liter flow or number setting) that you need (“oxygen prescription”) to keep your levels above 88%. If you desaturate below 89% with walking during this test without using oxygen, the therapist will check your oxygen levels while using oxygen at2 liters/minute (L/min), and if your numbers are not above 88%, they will walk you again using oxygen increased to4 L/min. The testing will continue until the correct liter flow of oxygen is determined that keeps your saturation at or above88-90%. This will be your oxygen prescription for you to use with exertion (walking, chores around the house, showering, ...).
- If your oxygen levels are below 89% at rest, you will also be prescribed oxygen at rest.
- Your physician may also ask for an overnight oximetry test to see if you desaturate during sleep.
Q. When should I use oxygen?
A. You should have a specific “Oxygen Prescription” from your physician for use of oxygen during rest, exercise, and/or sleep. If you are not clear about how much oxygen to use or when to use it, talk to your healthcare professionals to be clear on what liter flow or number settings you should be using with rest, exercise and sleep. If you only desaturate with exertion, then you will only use it with exercise. If your oxygen levels are always low, even while sitting quietly, then your physician might prescribe oxygen to be worn around the clock.
Q. How can I check my oxygen levels at home?
A. You can monitor your oxygen levels at home using a pulse oximeter, which can be purchased online or in a pharmacy without a prescription. Unfortunately, insurance does not cover them.
Q. What types of oxygen equipment will I use?
A. It is important to be informed about the different options for oxygen equipment to use at home and when you are out of the house -you can review additional resources here and also discuss with your health care provider and your oxygen provider. It is also very helpful to talk with other patients who use supplemental oxygen to see what works for them and to learn about how they use their different types of equipment. Some oxygen companies (referred to as DMEs-Durable Medical Equipment providers) offer different types of equipment so you might need to do a bit of 'shopping around' if you have specific needs, for example, if you work and will need oxygen all day at the office, or if you travel frequently, or if you have many levels of stairs in your home.
Q. What are the benefits of using oxygen?
A. The physiologic benefits of using supplemental oxygen (improved survival, prevention of pulmonary hyptertension, fewer hospitalizations) have not been well studied in patients with ILD. There is historical (1980) data supporting oxygen's benefit for severe emphysema patients, but we do not have that same data available for ILD patients. Some studies in ILD patients have documented increased activity levels and less breathlessness, however the reported benefits of using oxygen vary greatly among ILD patients. Some do not report significant improvement in their shortness of breath when using supplemental oxygen, while other patients report that using oxygen with exertion allows them to exercise more, prevents rapid and pounding heart rhythms, decreases cough, and allows them to get out of the house more often and have a more active lifestyle. If you have been prescribed oxygen by your physician it is important to discuss what you should reasonably expect and also to have a follow up appointment after you start using oxygen to be re-evaluated.
Participating in an ILD support group will help you adjust to life with oxygen as you can talk with others who use oxygen to get their tips and experiences. We encourage patients to follow their doctors' instructions on oxygen use, but only after a careful discussion between you and your physician about the expectations for its benefit. Your use of oxygen should be reviewed every visit and it is important to bring your portable oxygen with you to each visit.
Q. What if I am prescribed oxygen but choose not to use it?
A. Some patients with only mildly decreased oxygen levels may not feel less breathless or find that they can be more active when using oxygen. For others, use of oxygen may result in a significant improvement in the ability to exercise and get out of the house, work, and travel. If your physician recommends oxygen based on your testing results and you decide not to use it, it is important to continue to follow up with your healthcare team and be re-tested regularly (every 3-6 months). Your physician might also order an echocardiogram to evaluate your heart function and to see if low oxygen levels are causing some right heart strain and pulmonary hypertension. If you have low oxygen levels at rest, it is particularly important to use oxygen as prescribed as not doing so may put a greater strain on your heart.
Q. How do I know if I am getting enough oxygen?
A. Patients should try to maintain their oxygen saturation level above 88-90% throughout the day and night. Finger pulse oximeters (available over the counter in many pharmacies) allow for monitoring of oxygen levels at home or on the go. Just as diabetic patients check their blood sugar throughout the day and adjust their insulin dose to optimize their blood sugar level, ILD patients should similarly monitor their oxygen levels as directed by their healthcare providers. Once you have checked your levels with various activities, you do not need to check so frequently, but only if you feel a change in your symptoms.
Palliative Care refers to the management and treatment of the physical, intellectual, emotional, social, and spiritual needs of patients and their families and caregivers. Palliative Care can begin at the time of your diagnosis - it can proceed alongside the medical treatment for your ILD. The focus of Palliative Care is to provide support and strategies to relieve breathlessness, anxiety, or any other distressing symptoms that you may have. Our Palliative Care team also provides guidance on completion of advanced care planning such as POLST forms, Advanced Directives, and Durable Power of Attorney.
Hospice Services are designed to support patients and their families at the end of life, typically when it is estimated that a patient may have less than six months to live. The transition to hospice means that the focus of care is on quality and not quality of life. Medical management transitions to supportive care aimed at symptom relief as opposed to disease treatment. The benefits of hospice care include improved symptom management, practical and emotional support to families, access to medical equipment, and availability of a hospice nurse 24 hrs./day. Hospice services are most commonly provided in the home.