

Welcome to the Giaccia Laboratory
Research Overview
Dr. Amato Giaccia, Lab Director
My research program is focused on translating basic science findings on the role of hypoxia in tumor progression and resistance to therapy to pre-clinical models of cancer that we ultimately hope to take into the clinic. Our overarching hypothesis is that hypoxia not only makes tumor cells resistant to radiotherapy, chemotherapy and in some cases targeted therapy, but also increases their invasiveness and metastatic potential by inducing a select group of genes involved in tissue remodeling. We are rigorously investigating the genomic response of tumor cells to hypoxia and are developing new targeted therapies to eliminate hypoxic cells or inhibit the secreted gene products of hypoxic cells that drive malignant progression and metastasis. We have advanced understanding of gene regulation under hypoxic conditions, used synthetic lethal screening to identify new targets for hypoxia directed therapies, and are developing new diagnostics for hypoxia. Our future goals will be to further define critical effectors of the hypoxic response that are essential for tumor growth and expansion that can be targeted therapeutically.
KEYNOTE LECTURE: IS THE TUMOR MICROENVIRONMENT AN IMPEDIMENT TO THERAPY?
Ongoing Projects
- The frequently altered expression of metabolism genes in solid tumors such as clear cell renal cell cancer (ccRCC) has reinforced the importance of dysregulated metabolism in driving tumor expansion. Indeed, constitutive activation of the hypoxia inducible transcription factor (HIF) through mutations in the von Hippel Lindau (VHL) tumor suppressor gene or through exposure to hypoxia, results in enhanced glucose uptake, glycolytic flux, lactate secretion and suppression of mitochondrial activity. Conversely, reactive oxygen species produced by the mitochondria stimulate HIF-dependent transcription, creating an intricate signaling loop that balances mitochondrial oxygen consumption with the cellular response to hypoxia. In addition to stimulating glycolysis while suppressing OXPHOS, hypoxia has also been demonstrated to stimulate de novo lipogenesis through reductive glutamine metabolism, although it has not yet known how this reductive glutamine metabolism contributes to lipid accumulation in solid tumors and the clear cell phenotype in ccRCC. Importantly, HIF-dependent metabolic changes have been exploited therapeutically, indicating that a more comprehensive understanding of HIF regulated metabolism may yield novel anti-cancer therapies. Oxidative metabolism, which broadly encompasses carbohydrate oxidation, glutamine oxidation, and fatty acid β-oxidation, is controlled by a number of nuclear and mitochondrial transcription factors that together promote the biogenesis and enzymatic function of mitochondria and is often found repressed in many tumors including ccRCC. Our recent studies indicate that PGC-1α is suppressed in ccRCC through a HIF-α/Dec1 transcriptional axis. The suppression of PGC-1α in VHL-wild type renal proximal tubule cells is associated with reduced mitochondrial activity and acquisition of the clear cell (lipid and glycogen accumulation) phenotype, a histological hallmark of ccRCC. These findings provide the first evidence linking the clear cell phenotype to multiple aspects of renal tumorigenesis and raise the potential for PGC-1α stimulation as a novel therapeutic modality in the treatment of renal cell carcinoma, and potentially other solid tumors. Our goals are to explore the molecular mechanisms governing lipid homeostasis in cancer and to characterize their contribution to tumorigenesis and identify ways that they can be therapeutically targeted.
A patient presents with a primary pancreatic tumor that has metastasized to the liver. The liver is completely infiltrated with metastasis, and ultimately the metastasis will prevent the liver from functioning, and death will ensue. This is a frustrating situation, because we know where the metastases are located, we can image them, and attempt to treat them with cytotoxic chemotherapy. Unfortunately, chemotherapy only inhibits the metastasis in a short-term manner, and rarely eradicates the disease. Unlike chemotherapy, radiotherapy is highly effective in eradicating tumors, but it cannot be used to treat widespread metastasis in the liver due to normal tissue toxicity, especially at the doses of radiation needed to eliminate the metastasis. For radiotherapy to be used in such a manner, we need to develop effective radioprotectors that protect normal tissue, but not tumor tissue from radiation induced cell death. We have identified prolyl hydroxylase (PHD) inhibitors as promising agents that both stimulate erythropoiesis and protect the gastrointestinal tract from lethal doses of radiation without any effect on tumor radiosensitivity. Such agents will revolutionize the use of radiation for the treatment of metastasis, and most importantly would start to increase the long-term survival of patients with metastatic disease. So, our big idea for the next ten years is the normal tissues from radiation-induced lethality. This is a completely different approach to the treatment of metastatic disease that is risky, but would be revolutionary.
Targeting AXL
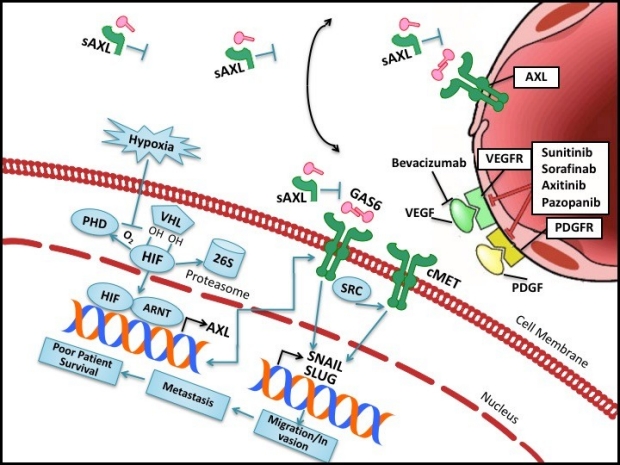
Clear cell renal cell carcinomas (ccRCC), the most common kidney cancers, are highly vascularized tumors that initially respond to antiangiogenic therapies. However, in the majority of patients treated with these agents, the tumor becomes resistant and progresses. Thus, therapies that inhibit additional molecular targets are needed to improve the overall survival rate of patients with metastatic ccRCC patients. We recently discovered that the receptor tyrosine kinase, AXL, is in part regulated by the von Hippel Lindau (VHL) tumor suppressor in ccRCC cell lines. Most importantly, AXL expression in ccRCC patients correlates with the lethal phenotype, strongly indicating an important role for AXL in the pathogenesis of ccRCC. In addition, AXL is an upstream regulator of both SRC and cMET signaling which are independent prognostic factors for poor survival in ccRCC patients. Genetic and pharmacologic inhibition of AXL signaling is sufficient to inhibit ccRCC tumor invasion and metastasis. While these findings establish an important biologic role for AXL in renal metastasis, there is a significant deficit of therapeutic agents that specifically target AXL signaling in the clinic. For this purpose, we produced an ultra-high-affinity soluble AXL (sAXL) FC-fusion protein. In our preclinical studies, we demonstrated that sAXL is a potent and selective inhibitor of GAS6 and is safe in mice. Furthermore, sAXL blocked GAS6 mediated signaling and tumor cell invasion and produced antitumor efficacy in multiple tumor models. We hypothesize that sAXL, an anti-metastatic agent, will be effective in treating sunitinib sensitive and resistant ccRCC and work in combination with antiangiogenic agents to enhance antitumor efficacy in ccRCC. Our goal is to investigate the efficacy, survival benefit, and safety of sAXL alone or in combination with immune therapy to support its clinical development for the treatment of advanced ccRCC.