Clinical Trial in a Dish:
A novel strategy for drug development in heart disease
by Amanda Chase, PhD
July 29, 2020
Dilated cardiomyopathy (DCM) is a disease of the heart muscle that results in decreased function of the left ventricle, the main pumping chamber. This decreases the heart’s ability to pump blood, which can lead to irregular heartbeats (arrhythmias), blood clots, heart failure, or sudden cardiac death. While there are several contributing factors to the development of DCM, it is known that up to one-third inherit it from their parents: familial DCM. Familial DCM is known to be caused by changes in different genes, the most common being variants (mutations) in the gene that encodes what is known as lamin A and C (LMNA); DCM caused by these variants is usually referred to as cardiolaminopathies. Although LMNA-associated DCM (or cardiolaminopathy) accounts for 6% of all familial cases, there are no targeted drug to prevent onset or progression of the disease, and the mechanisms that result in the cardiolaminopathy are not known.
Looking beyond the heart
Stanford Cardiovascular Institute scientists, Nazish Sayed, MD, PhD, and Joseph Wu, MD, PhD, Director of the Cardiovascular Institute, addressed both important needs in a paper recently published in Science Translational Medicine. They reasoned that as lamins are expressed in all differentiated cells, and dysfunction of non-myocytes such as endothelial cells (ECs) can contribute to the progressive failure of the heart muscle, there is opportunity to understand heart disease by looking beyond the heart muscle. They studied a large family cohort spanning four generations that had LMNA-associated DCM. Induced pluripotent stem cells (iPSCs), adult blood cells that were reprogrammed into stem cells, made from this family (members with DCM and healthy controls) allowed researchers to directly address questions of mechanism, especially in the tissue lining blood vessels and heart (endothelium). As iPSCs can be turned into any other kind of cells, the team generated iPSC-derived endothelial cells (iPSC-ECs) and were able to show and confirm a direct link between the change/mutation in the LMNA and the narrowing of large blood vessels (endothelial dysfunction). Narrowing of blood vessels contributes to decreased ability to pump blood.
Teaching old drugs, new tricks
Using next-generation sequencing, Stanford CVI researchers were able to identify a protein, Krüppel-like Factor 2 (KLF2) that plays a crucial role in mediating EC dysfunction in these recruited cardiolaminopathy family members. With the target identified, the team leveraged the iPSC platform to conduct a "clinical trial in-a dish" to identify drugs that could alleviate their observed clinical EC dysfunction. Importantly, they found that lovastatin, a 1st-generation statin, can help restore endothelial cell function in cells by increasing the expression of KLF2. “This was a significant discovery as it allowed us to repurpose lovastatin, an already FDA-approved drug for cardiolaminopathy and allowed us to move from cells to patients”, said Dr. Wu. Two members of the LMNA family were recruited, and the therapeutic effects of lovastatin were tested for up to 18 months. They found that as early as six months after starting oral lovastatin regimen, both the patients showed improvement in their clinical endothelial function.
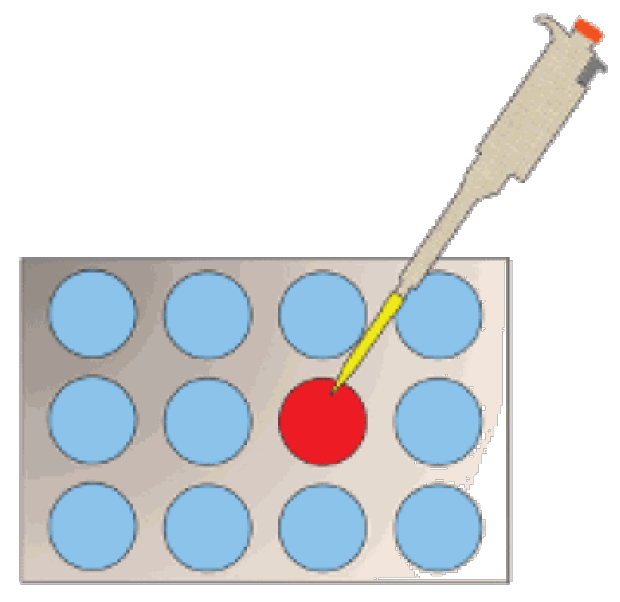
Clinical trials in-a dish: A revolutionary strategy for drug development, for drug safety, and for precision medicine using human tissues.
Fixing the plumbing
Similar to the plumbing in our house, the human body has an intricate piping system that is directly or indirectly connected to the heart, carrying blood to and from the heart. From the time when Leonardo da Vinci sketched the first diagram showing the distribution of the heart and its blood vessels in the fifteenth century, it is well established that the vasculature, lined by the endothelium as a diaphanous film of tissue, make for a vast network of pipes, which when damaged or dysfunctional, can lead to heart problems. “With this analogy in mind, we used our iPSC platform to test whether improving EC function in LMNA iPSC-ECs can improve heart muscle function for these patients”, said Dr. Sayed. First, the team tested this in-a dish and found that lovastatin treatment of LMNA endothelium improved function of LMNA heart cells when cultured together by improving the contractile properties of the heart muscle. Next, they tested this in patients, but found that even though lovastatin improved EC function in these patients, it failed to reverse the already set-in cardiac pathology. However, this does lend the intriguing possibility that improving endothelial cell function with lovastatin at an early stage, prior to cardiac symptoms, could delay onset of LMNA-associated DCM.
This Science Translational Medicine paper has important findings for understanding and treating a common form of DCM, and provides a potential therapeutic for delaying progression. Equally important, they demonstrate a workflow for identifying and validating potential drug treatments or patients that includes iPSCs (clinical trial in-a-dish) and patients.
Other Stanford Cardiovascular Institute authors include co-first author Chun Liu, Mohamed Ameen, Farhan Himmati, Joe Zhang, Saereh Khanamiri, Jan-Renier Moonen, Alexa Wnorowski, Linling Cheng, June-Wha Rhee, Karim Sallam, Jack Boyd, Joseph Woo, and Marlene Rabinovitch. Sadhana Gaddam and Kevin Wang are additional Stanford University authors. Funding was provided by NIH R01 HL130020, R01 HL1120006, R01 HL123968, R01 HL141851, R01 HL126527, and K01 HL135455; AHA Scientist Development Grant 13SDG17340025 and AHA Career Development Award 19CDA34760019; and Stanford TRAM scholar award.

Dr. Nazish Sayed
Dr. Chun Liu

Dr. Joseph Wu