Dementia Care
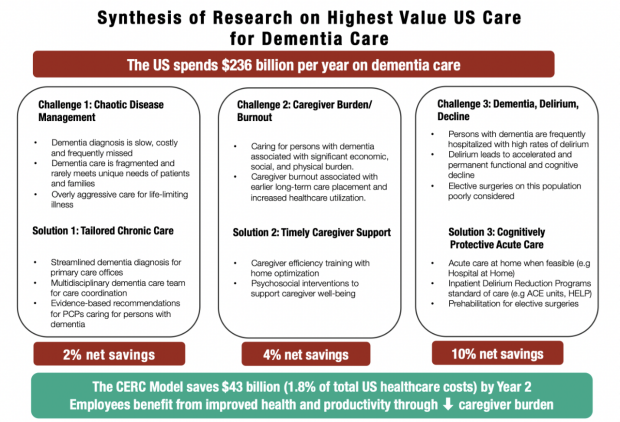
Dementia is the sixth leading cause of death in the United States and ranks fifth among individuals 65 years of age and older. With the rapid rise in the US population over 65, the prevalence of dementia in the US is expected to increase by 8.4 million by 2030. Alzheimer’s disease, the most common form of dementia in the US, today costs $236 billion in direct health care and long-term care costs.
How can the U.S. bring down the exploding cost of dementia care while substantially improving its quality and effectiveness? The CERC fellowship team set out to answer this question.
Projects and Outcomes
The potential savings the team uncovered were significant. The innovative model improves the quality of care while reducing total per capita annual health care spending by more than 15%, lowering the cost of health care for dementia patients by $42.6 billion within two years. The model achieves this in three ways: Through tailored chronic care, timely caregiver support, and cognitively protective acute care.
Tailored Chronic Care. Individuals with dementia are supported by a multidisciplinary care team led by a care navigator that functions as the primary point person for the patient and family. The model makes evidence-based recommendations to the primary care physician that include rethinking routine cancer screening and reducing the intensity of treatment for existing chronic diseases such as kidney diseases or diabetes.
Timely Caregiver Support. Improving efficiency at the start of caregiving can reduce the burden on the caregiver. This includes early home-based interventions such as visits by occupational therapists, which can ultimately reduce the caregiving hours required. Other recommended interventions are focused on caregiver efficiency training and support of caregiver wellbeing.
Cognitively Protective Acute Care. Identifying alternatives to hospitalization, particularly through the use of “hospital at home” whenever feasible. When this isn’t possible, the model recommends the use of inpatient delirium prevention programs, such as the Hospital Elder Life Program (HELP).
Overall, the proposed Care Model could lower the cost of dementia care in the United States by $42.6 billion within two years, representing total per member per year savings of 15.6%. Additional savings of approximately $1 billion could be realized from reduction of unpaid caregiving hours required by caregivers.