Ambulatory Surgical Care
Ambulatory surgical care currently accounts for 8% of domestic healthcare spending. It is a sector that is experiencing one of the fastest rates of growth, and it is delivered in a highly inefficient manner; furthermore, there is striking potential to improve the patient experience.
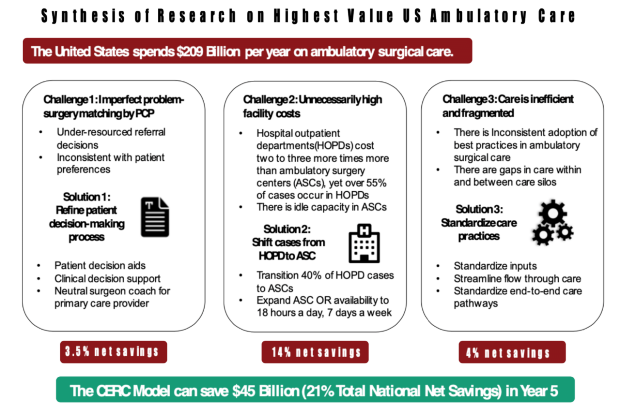
CERC’s surgical care redesign team found three addressable failure points in current methods of delivery of ambulatory surgical care. Team members addressed these failure points via a new care model with three core element.
- To reduce unnecessary or unwanted surgeries, primary care physicians consult with specialty-relevant physician and engage the patient in shared decision-making before patients are referred for ambulatory surgery to estimate for the patient the likely degree of improvement and risk of surgical complications.
- Consistent with surgical level of care standards widely employed in the UK and EU countries, most non-urgent outpatient surgeries for patients without major surgical risk factors are provided in free-standing ambulatory surgical centers.
- Freestanding ambulatory surgical centers operating at least 2 shifts/6 days per week apply systems engineering tools to safely maximize patient flow via standardized clinical pathways from pre-admission through post-admission care.
Projects and Outcomes
Net Percent reduction in total annual American health care spending: 1.25%
A conservative estimate of national savings from full implementation of the CERC surgical model is $45 billion per year in direct health care spending by the end of year five, or 21% of annual domestic spending on outpatient surgical care.