Fast Pediatric MRI Protocols
(S. Holdworth)
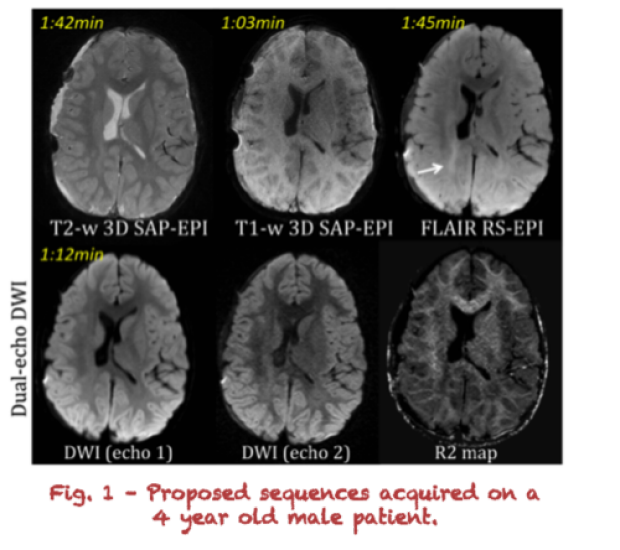
MRI provides excellent contrast between the different soft tissues of the body, which makes it especially useful in imaging brain pathology. The main disadvantage of MRI is that is lengthy, and can take up to one hour at our institution – due to the need for the rescanning of motion-corrupted exams. Particularly in a pediatric setting, long protocols increases the risk of motion artifacts in the acquired images, thus general anesthesia is often used – at the expense of patient throughput, comfort, and cost. With the goal of shortening the overall scan time of pediatric MRI, we are working on four MRI methods that have been built in-house and that can be retrospectively corrected for patient motion: a T1-weighted 3D Short-Axis Propeller Echo Planar Imaging (SAP-EPI) sequence1; a T2-weighted 3D SAP-EPI sequence2, a Fluid Attenuated Inversion Recovery (FLAIR) sequence using the Readout-Segmented (RS)-EPI trajectory3; and a dual-echo Diffusion-Weighted-Imaging (DWI) sequence4. The first three of these methods are faster than their conventional counterparts; and the latter can also deliver relaxivity (R2) maps.
Figure 1 shows preliminary images showing the promise of these research sequences – which together generate some of the leading contrast mechanisms required for pediatric brain imaging. Images are acquired on a 4 years old patient with prior resection of a right temporal lobe glioblastoma. Together the four sequences take 5:42min for whole brain coverage – faster than the sum of their conventional alternatives scanned at our institution (totaling ~14min). Currently we are working on technical developments that will bring this scan time down to ~3min, as well as on integrating these sequences with retrospective motion-correction. We will then investigate whether these sequences have the diagnostic potential to replace the need for the longer scan protocol acquired at our institution in the pediatric setting.
References: [1] S.J. Holdsworth et al. In: ISMRM #1239, 2009. [2] S.J. Holdsworth et al. JMRI (In Press) [3] S.J. Holdsworth et al. In: ISMRM #824. 2014 [4] S.J. Holdsworth et al. AJNR, In press.