Competition
The only existing retinal prosthesis approved for implantation in the US (2013) is the Second Sight Argus II. With it, people with certain types of blindness can detect large objects, the presence of people or cars, and sometimes oversized numbers or letters. Several others groups and companies are pursuing investigational efforts to develop retinal prosthetics, including Pixium Vision (France), Bionic Eye Technologies (US), and Nanoretina (Israel).
The current state of the art of retinal prostheses can be summed up as such: no blind patient today would trade their cane or guide dog for a retinal implant. Our goal is to build a device that can provide a high-fidelity, useful, and compelling visual experience, and indeed that approaches normal visual function as closely as the disease state of the patient will permit.
Indiscriminate vs. cell-type specific stimulation
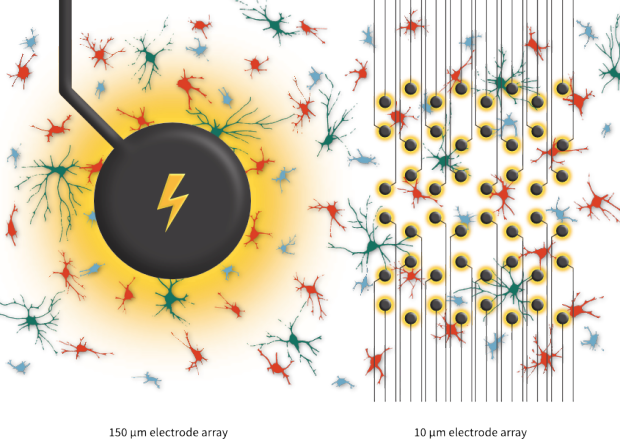
Present-day retinal implants stimulate the cells of the retina using large electrodes, typically 50-500 μm in diameter. Even though such devices have been successfully implanted in blind patients, the resulting experience of artificial vision remains limited. A major reason for this is that passing current through large stimulating electrodes results in the simultaneous activation of many ganglion cell types. This produces severely distorted patterns of activity in the retina, which in turn provide confusing and conflicting information to the brain. For example, simultaneous activation of ON and OFF type cells sends a “message” to the brain that both a light increase and a light decrease has occurred at the same retinal location at the same time. It is not surprising, therefore, that present-day devices produce very limited visual function.
This coarse and indiscriminate electrical stimulation contrasts with our approach, in which electrodes are approximately the same size as the cells they are intended to stimulate (around 10 μm). This allows each electrode to activate one or a small number of cells. Because each electrode is also capable of recording neuronal signals, the different ganglion cell types can be distinguished from one another and the physiologically correct stimulation signal be sent to each cell, and each cell type, individually.
Subretinal vs. epiretinal implants
A retinal implant can be placed on the retinal surface either on the side facing ganglion cells (epiretinal space) or on the side where photoreceptors were prior to degeneration (subretinal space).
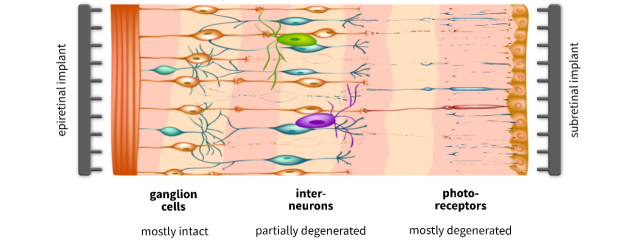
Present-day implants include both epiretinal (Second Sight Argus II, Pixium Vision IRIS) and subretinal (Pixium Vision PRIMA, Bionic Eye Technologies) approaches. Subretinal prostheses are easier to surgically maintain in place and offer the potential to stimulate any surviving outer retinal circuitry. They cannot, however, offer close proximity to ganglion cells. Due to this limitation, a subretinal implant is incapable of recording ganglion cell activity, a crucial requirement for reproducing the normal patterns of retinal activity. Our device is placed on the epiretinal surface to both records and directly stimulates individual ganglion cells.
Axon activation and the retinal raphe
All existing epiretinal prostheses face one highly problematic obstacle to high- resolution artificial vision: unwanted activation of ganglion cell axons. Because the retinal output projecting to the brain travels in the same plane as the electrode array, any electrode targeting ganglion cells has the potential to also activate passing axon bundles. Epiretinal implants such as the Second Sight Argus I and II have demonstrated that axonal activation leads to perceptual artifacts that are incompatible with faithfully reproducing visual sensations in blind patients. To combat this problem, we are proposing two solutions unique to our approach.
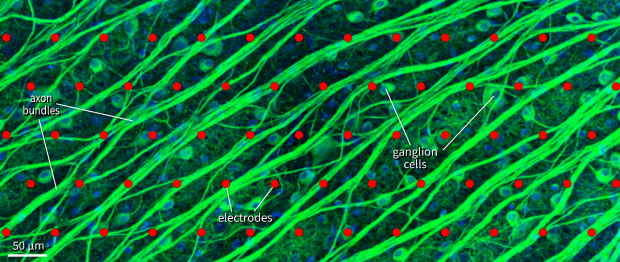
Ganglion cells and axon bundles (green) in primate retina during a 512-electrode recording and stimulation experiment.
First, we have used our laboratory artificial retina prototype to measure and quantify axon activation and discovered that it can be avoided by careful calibration of stimulation current levels and spatial electrode patterns. Due to the high number of available electrodes, our algorithm can steer clear of activating the electrodes near the biggest axon bundles.
In addition, we are targeting an area of the central retina that contains the lowest density of axon bundles. By placing the implant in the retinal raphe area, we can minimize unintentional axon activation while still producing high-acuity artificial vision.
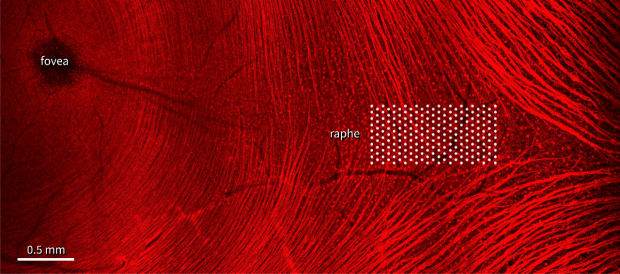
Human retina near the center-of-vision (fovea) contains a region where ganglion cell axon bundles (red) are sparse. We are placing our electrode array in this area.